Semaglutide vs tirzepatide which is better for weight loss
Semaglutide vs tirzepatide which is better for

Quick Answer
Retatrutide and tirzepatide are both incretin-based research compounds developed by Eli Lilly, but they differ fundamentally in receptor coverage. Tirzepatide is a dual GLP-1/GIP receptor agonist, currently FDA-approved and available clinically. Retatrutide adds a third mechanism, glucagon receptor activation, and in Phase 3 trials has demonstrated approximately 28% average body weight reduction over 18 months, compared to tirzepatide’s 22.5% in its own Phase 3 programme [1][2]. Retatrutide vs tirzepatide weight management research represents one of the most closely watched comparisons in metabolic science in 2026.
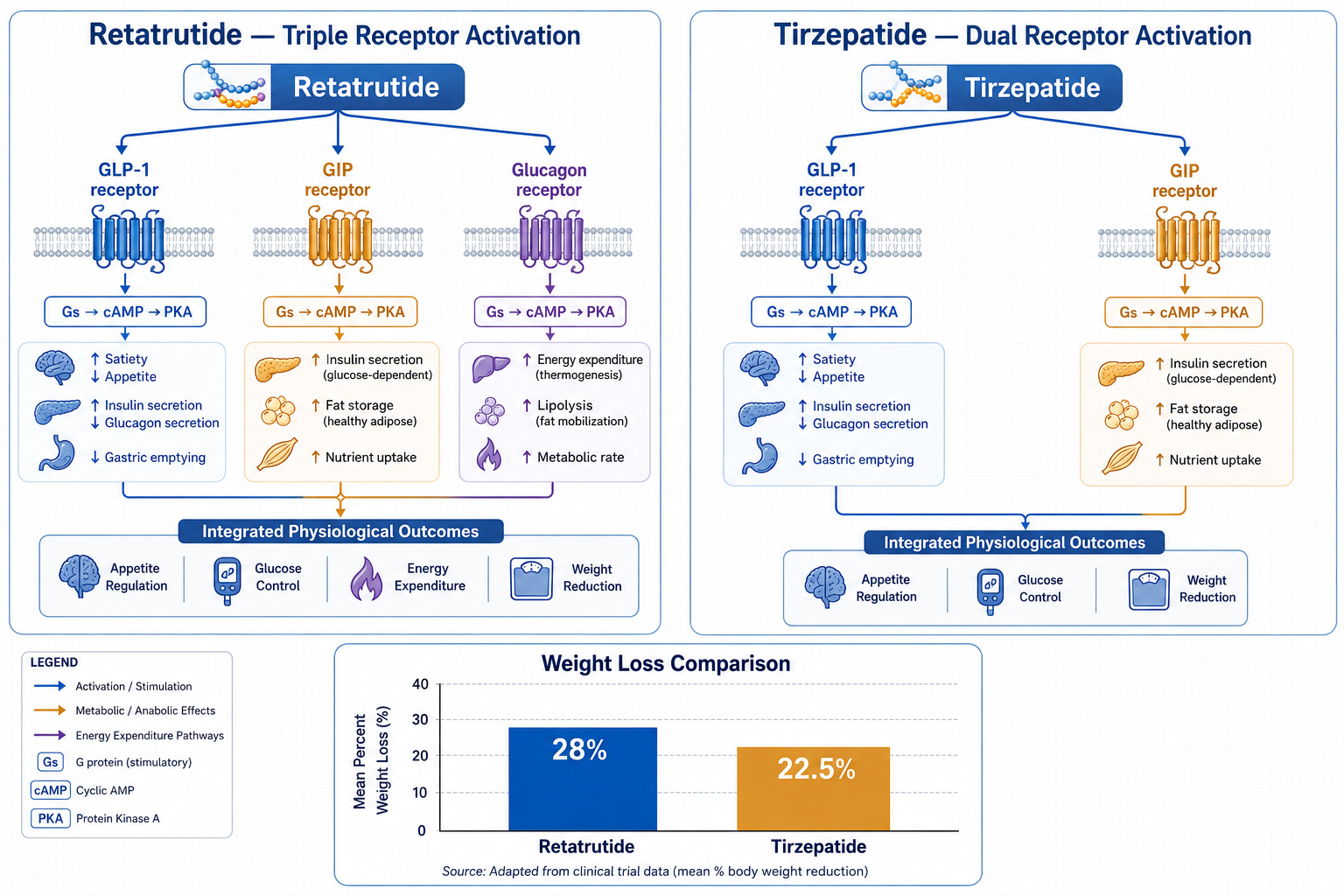
Retatrutide (also designated LY3437943) is a synthetic 39-amino acid peptide that simultaneously activates three receptor pathways: GLP-1 (glucagon-like peptide-1), GIP (glucose-dependent insulinotropic polypeptide), and the glucagon receptor. This triple-agonist mechanism distinguishes it from every currently approved incretin-based compound. Its approximate half-life of five days supports once-weekly subcutaneous administration in research protocols.
The GLP-1 component reduces appetite signalling in the hypothalamus and slows gastric emptying. The GIP component enhances insulin secretion and contributes to adipose tissue metabolism. The glucagon receptor component is the key differentiator: glucagon activation increases energy expenditure and promotes lipolysis, meaning the body is pushed toward burning stored fat at a rate that neither semaglutide nor tirzepatide can replicate through their respective mechanisms alone [1].
For qualified research professionals investigating advanced metabolic models, retatrutide’s triple-pathway activity makes it a structurally distinct compound from tirzepatide. Researchers exploring this area may also find the broader GLP/GIP multi-pathway metabolic research peptides overview a useful reference for contextualising receptor agonism research.
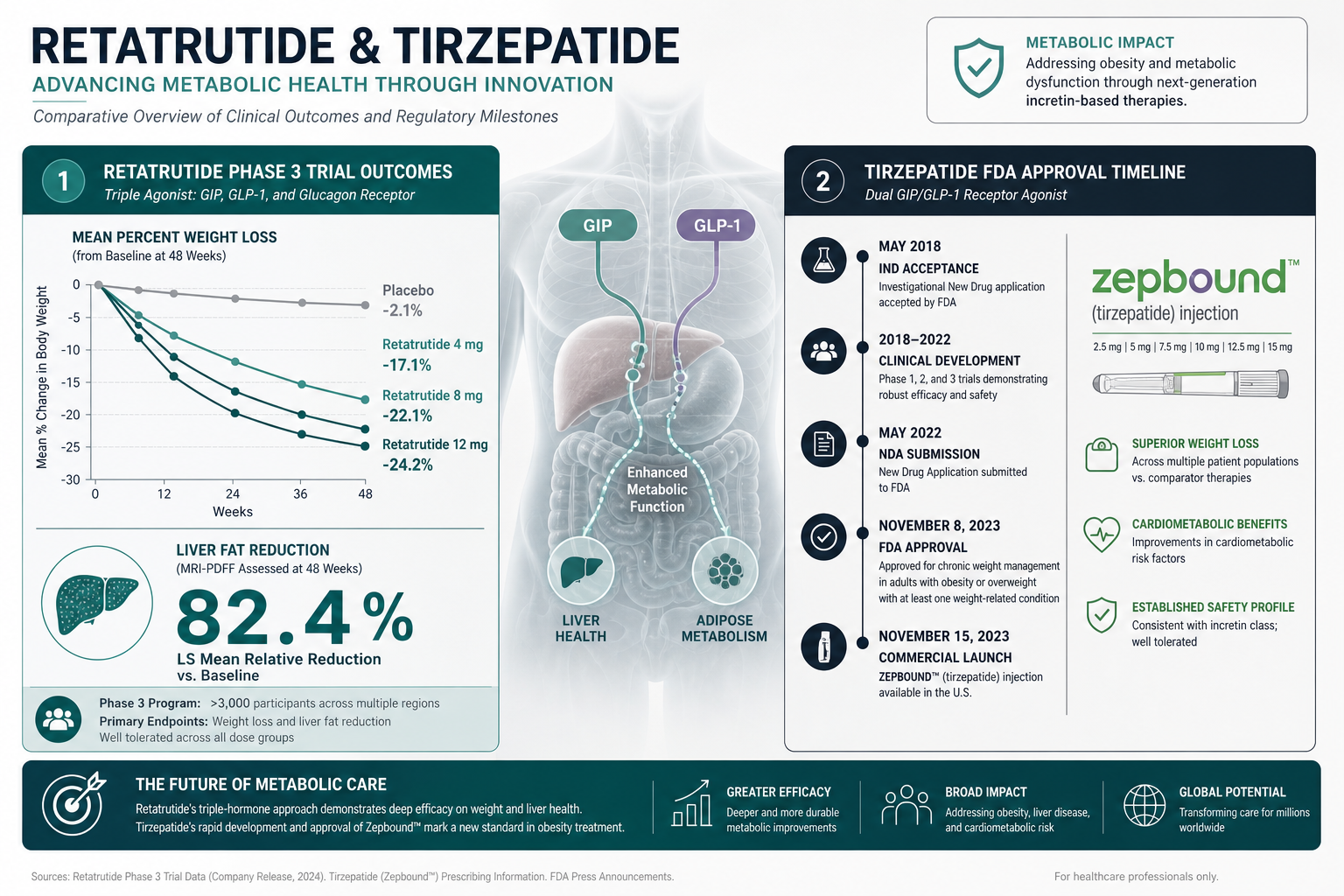
Phase 3 clinical trial data places retatrutide’s average body weight reduction at approximately 28% over 18 months, a figure that Eli Lilly and independent commentators have described as comparable to outcomes typically associated with bariatric surgery [2]. Tirzepatide’s SURMOUNT Phase 3 programme demonstrated up to 22.5% average weight loss.
To put these figures in concrete terms:
| Compound | Receptor Targets | Phase 3 Weight Reduction | Regulatory Status (2026) |
|---|---|---|---|
| Tirzepatide | GLP-1, GIP (dual) | Up to 22.5% | FDA-approved (Mounjaro, Zepbound) |
| Retatrutide | GLP-1, GIP, Glucagon (triple) | Approximately 28% | Investigational; Phase 3 ongoing |
| Semaglutide | GLP-1 (single) | Up to 15–17% | FDA-approved (Ozempic, Wegovy) |
The 5–6 percentage point difference between retatrutide and tirzepatide may appear modest in relative terms, but at population scale it represents a clinically meaningful separation. Eli Lilly has indicated plans to seek FDA approval for retatrutide pending successful completion of ongoing Phase 3 trials, potentially before the end of 2026 [2].
Semaglutide, marketed as Ozempic for type 2 diabetes and Wegovy for weight management, is a single GLP-1 receptor agonist. Both tirzepatide and retatrutide build on semaglutide’s foundation by adding receptor targets, which produces additive and in some cases synergistic effects on insulin secretion, appetite suppression, and energy metabolism [1].
The progression is straightforward: semaglutide targets one receptor pathway and achieves approximately 15–17% weight reduction in trials. Tirzepatide adds GIP agonism and reaches 22.5%. Retatrutide adds glucagon receptor activation on top of both and reaches approximately 28%. Each additional receptor target appears to contribute meaningfully to the overall metabolic effect, though it also introduces additional complexity in the side effect profile.
From a research perspective, this receptor hierarchy makes retatrutide vs tirzepatide weight management research directly relevant to understanding how incremental pathway additions translate into measurable metabolic outcomes. Researchers working with semaglutide as a baseline comparator can review what semaglutide is and how it works for foundational context.
Both retatrutide and tirzepatide produce gastrointestinal side effects as their most common adverse events, including nausea, diarrhoea, and vomiting. These effects are consistent across the incretin class and are generally dose-dependent, appearing most prominently during dose escalation phases.
Retatrutide carries one side effect not observed with tirzepatide: dysesthesia, a tingling or burning sensation reported in approximately 20.9% of participants receiving the 12 mg dose in Phase 2 trials [3]. The mechanism behind this is not yet fully characterised, though glucagon receptor activation in peripheral nervous tissue is a candidate explanation under investigation.
Glucagon receptor activation also raises a cardiovascular consideration. Retatrutide has been associated with increases in resting heart rate, which requires careful monitoring in research subjects with pre-existing cardiovascular concerns [1]. Tirzepatide does not carry this same degree of heart rate elevation signal.
Discontinuation rates due to adverse events are higher with retatrutide than with tirzepatide, reflecting the broader side effect burden that accompanies its greater efficacy [3]. This trade-off between potency and tolerability is a central consideration in ongoing Phase 3 evaluation.
Retatrutide’s research profile extends beyond body weight reduction. In participants with metabolic dysfunction-associated steatotic liver disease (MASLD), retatrutide demonstrated an 82.4% reduction in liver fat content [4]. This finding positions it as a compound of significant interest in hepatic metabolic research, a field where effective interventions have historically been limited.
This liver fat reduction likely reflects the combined action of GIP-mediated fat metabolism and glucagon-driven lipolysis, both of which reduce hepatic lipid accumulation through distinct but complementary mechanisms. Researchers investigating visceral adiposity alongside hepatic outcomes may also find the tesamorelin visceral fat research context relevant, as tesamorelin addresses visceral fat through a distinct growth hormone-releasing mechanism.
In clinical terms, tirzepatide is currently the only one of the two compounds available for prescription use, making it the accessible option for patients with type 2 diabetes or obesity meeting specific criteria. Retatrutide remains investigational and is not available outside of clinical trials or research settings.
From a research design perspective, the choice between compounds depends on the specific metabolic pathway under investigation:
Research professionals sourcing tirzepatide for laboratory use can access tirzepatide 30mg or tirzepatide 60mg through Sempica’s catalogue, while retatrutide 20mg and retatrutide 40mg are available for advanced metabolic research applications.
Neither retatrutide nor tirzepatide is appropriate for individuals with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 (MEN 2), based on preclinical signals observed across the GLP-1 receptor agonist class. Pancreatitis history is also a standard contraindication under clinical evaluation protocols.
For retatrutide specifically, the additional glucagon receptor activity introduces cardiovascular monitoring requirements that are less prominent with tirzepatide. Individuals with significant cardiac arrhythmia risk or elevated baseline heart rate require careful assessment before inclusion in retatrutide research protocols [1].
The key risks across both compounds include:
All compounds available through Sempica are strictly for research use by qualified professionals. They are not for human consumption, medical use, or therapeutic application.
Tirzepatide, as an FDA-approved medication, is commercially available by prescription in the United States under the Mounjaro and Zepbound brand names. List prices have been reported in the range of USD 1,000–1,100 per month before insurance or manufacturer discount programmes. Insurance coverage for Zepbound (the weight management indication) has been inconsistent, with many commercial plans applying prior authorisation requirements and some government programmes excluding coverage for obesity medications entirely.
Retatrutide has no commercial pricing established as of mid-2026, as it remains investigational. Access is currently limited to clinical trial enrolment and, for research purposes, through qualified laboratory supply channels. The commercial landscape will shift substantially if Eli Lilly secures FDA approval, which the company has indicated as a near-term objective [2].
For research procurement, Sempica supplies both compounds to qualified professionals globally. Researchers requiring guidance on compound preparation should consult the how to reconstitute tirzepatide 30mg guide and the broader how to calculate peptide dosage for research resource.
Weight maintenance after cessation of GLP-1 and incretin-class compounds is an active area of investigation. Published data from tirzepatide withdrawal studies indicate that a significant proportion of lost weight is regained within 12 months of stopping treatment, consistent with the broader pattern observed across the GLP-1 class. This reflects the pharmacological nature of the appetite and metabolic suppression: effects are present while the compound is active and diminish when it is withdrawn.
Retatrutide’s durability data beyond the 18-month Phase 3 window is not yet fully characterised. The glucagon receptor component, which drives energy expenditure, may offer a different durability profile compared to appetite-only mechanisms, but this remains a hypothesis under investigation rather than an established finding [5].
The obesity pharmacology field is increasingly focused on this durability question, with companies exploring combination therapies, extended-release formulations, and adjunct interventions to sustain long-term outcomes [5].
The data emerging from retatrutide and tirzepatide research collectively represents a significant shift in the ceiling of pharmacological body weight reduction. The approximately 28% weight loss demonstrated by retatrutide in Phase 3 trials challenges the historical assumption that bariatric surgery represents the upper limit of achievable weight reduction [2].
For metabolic research, this has several implications. First, it validates the multi-receptor agonism strategy: adding receptor targets produces measurable, incremental improvements in metabolic outcomes. Second, it raises the question of where the ceiling lies, and whether further receptor additions (such as amylin or FGF21 agonism, both under investigation in combination compounds) will continue the upward trend. Third, it focuses attention on the tolerability challenge: greater potency appears to come with a higher side effect burden, and the field must determine how to preserve efficacy while improving patient retention [5].
Researchers investigating these questions can also explore related metabolic compounds in the metabolic and energy research compounds catalogue, which includes MOTS-c and other compounds relevant to insulin sensitivity and mitochondrial metabolism research.
What is the main structural difference between retatrutide and tirzepatide?
Retatrutide is a 39-amino acid synthetic peptide with triple GLP-1/GIP/glucagon receptor agonism. Tirzepatide is a 39-amino acid synthetic peptide with dual GLP-1/GIP receptor agonism. The glucagon receptor component in retatrutide is the key structural and pharmacological distinction.
Is retatrutide FDA-approved in 2026?
As of mid-2026, retatrutide remains investigational. Eli Lilly has completed Phase 3 trials and has indicated plans to seek FDA approval, potentially before the end of 2026. Tirzepatide is FDA-approved under the brand names Mounjaro and Zepbound [2].
What percentage of body weight can be lost with retatrutide compared to tirzepatide?
Phase 3 data shows retatrutide achieving approximately 28% average body weight reduction over 18 months. Tirzepatide’s Phase 3 programme demonstrated up to 22.5% [2].
What is dysesthesia and why does it occur with retatrutide?
Dysesthesia refers to abnormal sensations including tingling or burning. It was reported in approximately 20.9% of retatrutide participants at the 12 mg dose in Phase 2 trials. The exact mechanism is not fully established but may relate to glucagon receptor activity in peripheral neural tissue [3].
Can retatrutide reduce liver fat?
Yes. In research participants with MASLD, retatrutide demonstrated an 82.4% reduction in liver fat content, suggesting significant hepatic metabolic activity beyond its weight loss effects [4].
Does tirzepatide affect the heart rate the same way retatrutide does?
Tirzepatide does not carry the same degree of resting heart rate elevation signal observed with retatrutide. The glucagon receptor activation in retatrutide is the likely driver of this cardiovascular consideration [1].
Which compound has a better tolerability profile?
Tirzepatide has a more favourable tolerability profile based on current data. Retatrutide’s higher discontinuation rate due to adverse events, combined with the dysesthesia signal, places a greater tolerability burden on participants compared to tirzepatide [3].
Are these compounds available for laboratory research?
Yes. Both tirzepatide and retatrutide are available as research compounds through qualified laboratory supply platforms such as Sempica, for use by qualified research professionals in controlled settings only. They are not for human consumption or therapeutic application.
How do these compounds compare to semaglutide?
Semaglutide (GLP-1 only) achieves approximately 15–17% weight reduction. Tirzepatide (GLP-1 + GIP) reaches approximately 22.5%. Retatrutide (GLP-1 + GIP + glucagon) reaches approximately 28%. Each additional receptor target adds measurable metabolic effect.
What happens to weight when these compounds are stopped?
Significant weight regain is observed after cessation of tirzepatide, consistent with the broader GLP-1 class pattern. Retatrutide’s long-term durability data post-cessation is not yet fully characterised. This remains an active area of research [5].
Retatrutide vs tirzepatide weight management research defines a critical frontier in metabolic pharmacology in 2026. The evidence is clear on the efficacy hierarchy: retatrutide’s triple-receptor mechanism produces greater weight reduction than tirzepatide’s dual-receptor approach, and both substantially outperform semaglutide. The 28% average body weight reduction observed in retatrutide’s Phase 3 programme, alongside an 82.4% reduction in liver fat in MASLD participants, positions it as the most potent incretin-based compound currently in late-stage development [2][4].
However, greater potency does not automatically mean a better research or clinical choice. Retatrutide’s higher side effect burden, the unique dysesthesia signal, cardiovascular monitoring requirements, and higher discontinuation rates are all factors that research protocols must account for [3]. Tirzepatide, as an FDA-approved compound with a well-characterised safety profile, remains the more accessible and better-understood option for dual-pathway metabolic research.
For research professionals, the actionable steps are:
[1] Retatrutide Vs Tirzepatide – https://www.protocolapp.health/research/articles/retatrutide-vs-tirzepatide?utm_source=openai
[2] Experimental Lilly Drug Surgery Level Weight Loss – https://www.axios.com/2026/05/21/experimental-lilly-drug-surgery-level-weight-loss?utm_source=openai
[3] Retatrutide Vs Tirzepatide – https://www.glp3.wiki/articles/retatrutide-vs-tirzepatide?utm_source=openai
[4] Retatrutide Vs Tirzepatide – https://peptideguide.com/compare/retatrutide-vs-tirzepatide/?utm_source=openai
[5] Obesity Drug Race Patient Benefits – https://www.axios.com/2026/06/03/obesity-drug-race-patient-benefits?utm_source=openai
Products sold on this website are intended for research purposes only. They are not for human consumption, medical use, or therapeutic application. By purchasing from this website, you confirm that you are a qualified professional and will use these products strictly for laboratory research.
Semaglutide vs tirzepatide which is better for
Confused on Retatrutide vs Tirzepatide for weight
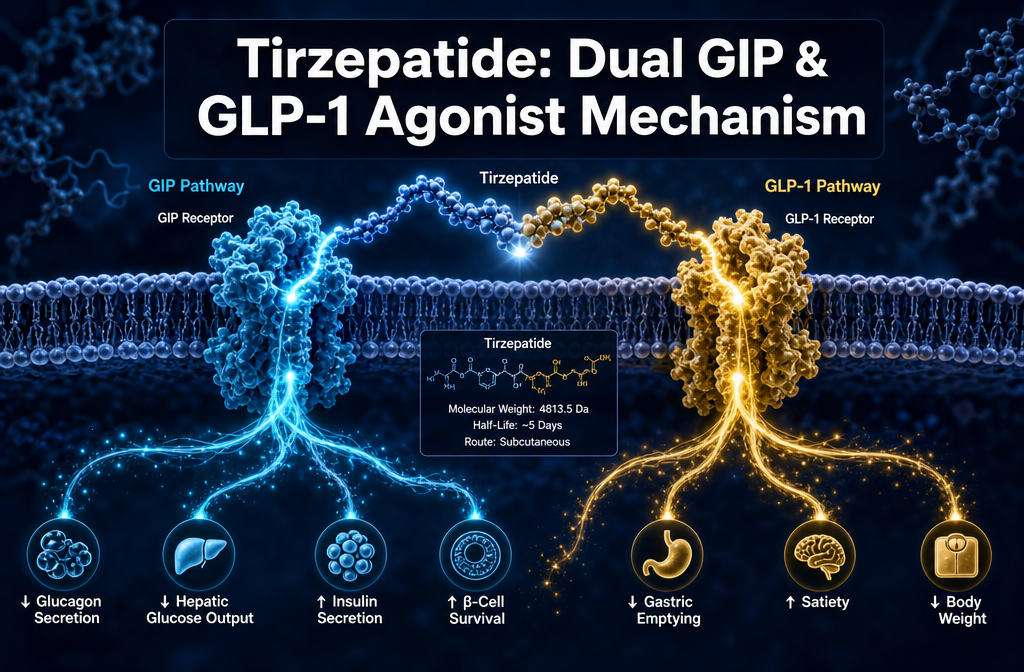
What is Tirzepatide dual GIP GLP-1 agonist