Semaglutide vs tirzepatide which is better for weight loss
Semaglutide vs tirzepatide which is better for
High-Purity Research Compounds | Trusted Quality & Consistency
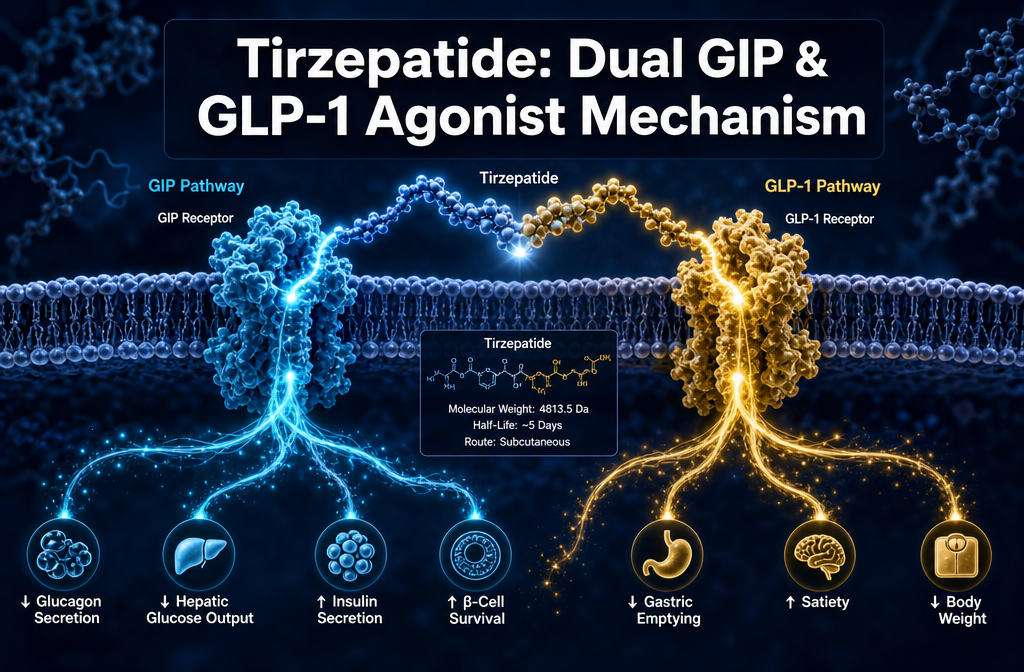
Quick Answer: Tirzepatide is a 39-amino acid synthetic peptide that simultaneously activates both the glucose-dependent insulinotropic polypeptide receptor (GIPR) and the glucagon-like peptide-1 receptor (GLP-1R). This tirzepatide dual GIP GLP-1 agonist mechanism produces additive effects on insulin secretion, glucagon suppression, and appetite regulation that exceed what single-receptor agonism achieves alone. It is approved for type 2 diabetes management and chronic weight management in adults with obesity or overweight with at least one weight-related comorbidity.
A dual agonist binds to and activates two separate receptor types at once, triggering both signalling pathways simultaneously. In the case of tirzepatide, this means activating GIPR and GLP-1R in the pancreas, gut, brain, and adipose tissue at the same time, producing coordinated metabolic effects that neither receptor pathway achieves independently.
When GLP-1R is activated, it stimulates insulin secretion in a glucose-dependent manner, suppresses glucagon release from pancreatic alpha cells, slows gastric emptying, and signals satiety through the hypothalamus. When GIPR is activated alongside it, additional insulin secretion is triggered, lipid metabolism in adipose tissue is modulated, and — critically — the nausea associated with GLP-1R agonism appears to be partially attenuated [1][5].
The combined signalling through both receptors elevates intracellular cyclic AMP (cAMP) levels more than either receptor pathway alone. This amplified cAMP response drives greater insulin granule exocytosis from beta cells and more pronounced suppression of appetite-regulating neuropeptides in the hypothalamus [2][4]. Research suggests that GIPR agonism in the central nervous system may independently reduce food intake, adding a second appetite-suppression mechanism on top of the GLP-1R pathway [5].
Tirzepatide occupies a distinct pharmacological class. Unlike metformin (which reduces hepatic glucose output), sulfonylureas (which stimulate insulin release independent of glucose), or SGLT-2 inhibitors (which promote renal glucose excretion), tirzepatide works through incretin hormone receptor activation, making its insulin-stimulating effects glucose-dependent and therefore carrying a lower intrinsic hypoglycaemia risk when used without insulin or sulfonylureas [6][10].
Compared with older GLP-1 receptor agonists such as liraglutide or exenatide, tirzepatide’s dual mechanism consistently produces superior glycaemic control and greater weight reduction. In the SURPASS clinical programme, tirzepatide demonstrated statistically significant superiority over semaglutide 1 mg in reducing HbA1c at 40 weeks [4].
The key differentiator is the GIP component. Earlier research questioned whether GIPR agonism would be beneficial, since GIP’s insulinotropic effect is blunted in established type 2 diabetes. However, preclinical and clinical data indicate that pharmacological GIPR agonism at the doses achieved with tirzepatide restores meaningful receptor responsiveness, and the combined receptor activation produces metabolic outcomes not achievable through GLP-1R agonism alone [1][2].
Tirzepatide and semaglutide share GLP-1 receptor agonism as a common mechanism, but they are structurally and pharmacologically distinct compounds.
Semaglutide is a 34-amino acid GLP-1 analogue that binds exclusively to GLP-1R with high potency. Tirzepatide is a 39-amino acid peptide engineered with a C20 fatty diacid moiety that enables it to bind both GIPR and GLP-1R. Importantly, tirzepatide’s affinity for GLP-1R is actually lower than semaglutide’s on a molar basis, yet it achieves superior clinical outcomes because the additive GIP receptor activation compensates and augments the overall metabolic response [2][5].
For a detailed comparison of the GLP-1 mechanism in isolation, the guide on what semaglutide is and how it works provides useful context on the single-receptor pathway.
| Feature | Semaglutide | Tirzepatide |
|---|---|---|
| Receptor targets | GLP-1R only | GLP-1R + GIPR |
| Amino acid length | 34 | 39 |
| Half-life | ~7 days | ~5 days |
| GLP-1R affinity | Very high | Moderate |
| GIPR affinity | None | High |
| HbA1c reduction (max dose) | ~1.8% | ~2.3% |
| Mean weight reduction (max dose) | ~14.9% (STEP-1) | ~20.9% (SURMOUNT-1) |
The practical implication for researchers is that tirzepatide’s dual mechanism provides a distinct experimental model compared with selective GLP-1R agonism. Studies comparing these compounds directly are central to understanding incretin biology. For researchers investigating multi-pathway metabolic compounds, the GLP-1/GIP multi-pathway metabolic research peptides resource outlines the broader research landscape.
In clinical research, tirzepatide has produced the largest mean weight reductions observed in any approved pharmacological agent for obesity to date. In the SURMOUNT-1 trial, participants without diabetes who received 15 mg weekly achieved a mean weight reduction of approximately 20.9% from baseline over 72 weeks, compared with 3.1% in the placebo group [9][10].
Results vary significantly by dose and individual response. Lower doses (5 mg and 10 mg) produced mean reductions of approximately 15% and 19.5% respectively in the same trial. These figures represent group means — individual responses range considerably based on baseline metabolic status, dietary adherence, and other factors [9].
For type 2 diabetes populations (SURPASS trials), weight reductions were somewhat lower, averaging 7–12 kg across dose groups, likely reflecting the metabolic differences between diabetic and non-diabetic subjects [4][10].
Important framing for research contexts: These outcomes are derived from controlled clinical trials with specific inclusion criteria, dosing protocols, and lifestyle intervention components. Translating these figures to individual predictions requires clinical assessment.
The most commonly reported side effects are gastrointestinal and are consistent with the GLP-1R agonist class. Nausea, diarrhoea, vomiting, and constipation are the most frequent, occurring most often during dose escalation phases [6][10].
In the SURPASS and SURMOUNT trials, gastrointestinal adverse events led to discontinuation in approximately 4–7% of tirzepatide-treated participants, depending on dose [10]. The gradual dose escalation protocol (typically starting at 2.5 mg and increasing by 2.5 mg every four weeks) is specifically designed to reduce the severity of these effects.
Less common but clinically relevant adverse events include:
The tirzepatide dual GIP GLP-1 agonist mechanism may actually reduce nausea relative to equipotent GLP-1R agonism alone. Preclinical data suggest that GIPR activation in the area postrema (a brainstem emesis centre) may counteract GLP-1R-mediated nausea signalling, which could partly explain why tirzepatide’s tolerability profile compares favourably in some analyses [5][8].
Tirzepatide has demonstrated strong efficacy in both indications, and regulatory approvals reflect this dual utility. It was first approved for type 2 diabetes management (as Mounjaro) and subsequently approved for chronic weight management in adults with obesity (as Zepbound in the United States).
For type 2 diabetes, tirzepatide consistently achieves HbA1c reductions of 1.8–2.3% from baseline, with a high proportion of participants reaching HbA1c targets below 7.0% [4][10]. For weight management, the magnitude of body weight reduction exceeds that of any previously approved pharmacological agent.
The more precise framing is that tirzepatide is not “better” for one indication over the other — it is highly effective in both. The clinical decision depends on the patient’s primary therapeutic need, existing medications, comorbidities, and individual tolerability.
For researchers comparing tirzepatide with next-generation triple agonists, the tirzepatide versus retatrutide research outcomes analysis examines how adding glucagon receptor agonism (as in retatrutide) may further extend metabolic research applications.
Tirzepatide is contraindicated in specific populations based on safety data from clinical trials and mechanistic considerations. This section reflects clinical contraindications relevant to human therapeutic use.
Absolute contraindications include:
Relative contraindications and populations requiring careful evaluation include individuals with a history of pancreatitis, severe gastrointestinal disease, diabetic retinopathy (rapid glycaemic improvement can transiently worsen retinopathy), severe renal impairment, and pregnancy or breastfeeding.
The thyroid cancer warning stems from rodent studies in which GLP-1R agonists induced C-cell tumours at suprapharmacological doses. Whether this risk translates to humans remains under investigation, and long-term pharmacovigilance data are still accumulating [10].
Emerging research suggests that tirzepatide may be relevant in prediabetes contexts. In the SURMOUNT-1 trial, a substantial proportion of participants had prediabetes at baseline. Among this subgroup, a high percentage reverted to normoglycaemia by the end of the trial period, suggesting that the compound’s mechanisms of improving insulin sensitivity and reducing body weight may interrupt the progression from prediabetes to type 2 diabetes [9][10].
This is an active area of investigation. The tirzepatide dual GIP GLP-1 agonist mechanism addresses two of the core pathophysiological drivers of prediabetes: impaired incretin response and insulin resistance in peripheral tissues. Whether early intervention produces durable glycaemic normalisation beyond the treatment period remains to be established in longer-term studies.
Glycaemic improvements (reductions in fasting glucose and postprandial glucose) are detectable within the first one to two weeks of treatment, as the incretin receptor activation begins modulating insulin and glucagon secretion from the first dose [6][10].
Meaningful weight reduction typically becomes apparent within four to eight weeks, with progressive reduction continuing throughout the dose escalation phase and beyond. The maximum therapeutic dose (15 mg) is generally reached at week 20 following the standard escalation schedule. Most clinical trials report the majority of total weight loss occurring within the first 36 weeks, with continued but slower reduction through week 72 [9].
Researchers should note that results in clinical trials reflect structured protocols with dietary and lifestyle components. The compound’s pharmacokinetic profile (half-life of approximately five days) means that steady-state plasma concentrations are reached after approximately four to five weeks at any given dose.
Several patterns consistently emerge in both clinical practice and research settings that reduce the quality of outcomes or increase adverse event rates.
Escalating dose too quickly is the most common error. The standard escalation schedule exists specifically to allow gastrointestinal adaptation. Accelerating beyond the recommended four-week intervals at each dose significantly increases nausea and vomiting rates and often leads to discontinuation.
Inadequate hydration management compounds gastrointestinal side effects. Diarrhoea and vomiting during initiation can cause dehydration, which in turn worsens tolerability.
Failing to account for drug interactions is a research and clinical concern. Tirzepatide slows gastric emptying, which can alter the absorption kinetics of orally administered medications taken concurrently, including oral contraceptives and some antibiotics.
In laboratory research contexts, improper reconstitution or storage is a frequent source of compound degradation. Tirzepatide research compounds should be stored as lyophilised powder at -20°C and reconstituted with bacteriostatic water using the correct technique. The guide on how to reconstitute tirzepatide 30mg provides a detailed protocol. Reconstituted solutions should be stored at 2–8°C and used within the validated stability window. For broader peptide storage guidance, see how long reconstituted peptides last in the fridge.
Discontinuation of tirzepatide does not produce acute withdrawal effects in the pharmacological sense. However, the metabolic benefits are not permanent — they are dependent on continued receptor activation.
Clinical data from the SURMOUNT-4 trial demonstrated that participants who discontinued tirzepatide after achieving weight loss regained approximately two-thirds of their lost weight within one year of stopping [9]. Glycaemic parameters (HbA1c, fasting glucose) also returned toward baseline values in the months following discontinuation.
This pattern reflects the underlying biology: tirzepatide does not correct the root causes of obesity or type 2 diabetes but rather modulates the incretin and appetite regulatory systems as long as the compound is present. When the receptor agonism ceases, the systems revert. This has significant implications for treatment planning and for research protocols studying sustained metabolic adaptation.
In the United States, the list price for branded tirzepatide (Mounjaro or Zepbound) ranges from approximately $900 to $1,100 per month at the time of publication, depending on dose and formulation. Actual out-of-pocket costs vary considerably based on insurance coverage, manufacturer savings programmes, and pharmacy pricing [9].
For laboratory research use, tirzepatide is available as a research compound at substantially different price points through qualified suppliers. Sempica Healthcare offers tirzepatide research compounds, including tirzepatide 30mg and tirzepatide 60mg, formulated to a 99.8% purity standard, independently verified by Certificate of Analysis, and supplied exclusively for research purposes.
Mandatory disclaimer: All tirzepatide products available through Sempica Healthcare are intended for research purposes only. They are not for human consumption, medical use, or therapeutic application. By purchasing from this website, you confirm that you are a qualified professional and will use these products strictly for laboratory research.
Long-term safety data for tirzepatide are still accumulating, given that the compound received its first regulatory approval in 2022. The available evidence from trials extending to 72–88 weeks provides a reasonable safety profile, but multi-year pharmacovigilance data are limited [10].
The most closely monitored long-term concerns include:
For researchers investigating the broader metabolic research compound landscape, the metabolic and energy research compounds resource provides context on related pathways under investigation.
What makes tirzepatide a “twincretin”?
The term “twincretin” refers to tirzepatide’s ability to activate both GIP and GLP-1 incretin hormone receptors simultaneously. No previously approved diabetes medication had achieved dual incretin receptor agonism in a single molecule before tirzepatide.
Does tirzepatide cause hypoglycaemia?
Tirzepatide’s insulin-stimulating effects are glucose-dependent, meaning they diminish as blood glucose normalises. Hypoglycaemia risk is low when tirzepatide is used as monotherapy but increases significantly when combined with insulin or sulfonylureas.
How is tirzepatide administered?
Tirzepatide is administered via subcutaneous injection once weekly. The standard starting dose is 2.5 mg, escalated by 2.5 mg every four weeks to a maximum of 15 mg.
Is tirzepatide approved for adolescents?
As of 2026, tirzepatide’s approved indications are for adults. Paediatric trials are ongoing, and regulatory decisions for younger populations have not yet been finalised in most jurisdictions.
Can tirzepatide be used in people with kidney disease?
Mild to moderate renal impairment does not require dose adjustment based on current pharmacokinetic data. Severe renal impairment warrants caution, and clinical guidance should be followed.
What is the difference between Mounjaro and Zepbound?
Both are brand names for tirzepatide. Mounjaro is approved for type 2 diabetes management; Zepbound is approved for chronic weight management. The active compound and formulation are identical.
How does the GIP receptor component reduce nausea?
Preclinical research suggests that GIPR activation in brainstem emesis centres may partially counteract the nausea-inducing effects of GLP-1R activation, contributing to tirzepatide’s comparatively favourable gastrointestinal tolerability profile relative to equipotent GLP-1R agonists [5][8].
Is tirzepatide available for research use?
Yes. Tirzepatide is available as a lyophilised research compound from qualified suppliers including Sempica Healthcare, formulated to 99.8% purity for use in laboratory research by qualified professionals only.
How does tirzepatide compare with retatrutide?
Retatrutide adds glucagon receptor agonism to the GIP/GLP-1 dual mechanism, creating a triple agonist with potentially greater effects on energy expenditure and lipolysis. Early clinical data suggest even greater weight reduction with retatrutide, though the long-term safety profile is less established. See the tirzepatide versus retatrutide research outcomes comparison for further detail.
What storage conditions are required for tirzepatide research compounds?
Lyophilised tirzepatide powder should be stored at -20°C, away from light and moisture. Reconstituted solutions should be stored at 2–8°C and used within the validated stability period. Never freeze a reconstituted solution.
The tirzepatide dual GIP GLP-1 agonist mechanism represents a meaningful advance in incretin pharmacology. By activating both GIPR and GLP-1R simultaneously, tirzepatide produces additive metabolic effects — greater insulin secretion, more pronounced glucagon suppression, amplified appetite reduction, and improved adipose tissue insulin sensitivity — that consistently outperform selective GLP-1R agonism in head-to-head clinical comparisons.
For research professionals, the actionable priorities are clear. Understand the mechanistic distinction between single and dual receptor agonism before designing comparative studies. Account for the compound’s five-day half-life and glucose-dependent insulin-stimulating properties when structuring experimental protocols. Ensure proper lyophilised storage at -20°C and follow validated reconstitution procedures to preserve compound integrity. When comparing tirzepatide with next-generation triple agonists such as retatrutide, recognise that each additional receptor pathway introduces distinct metabolic variables that must be controlled for.
For those sourcing tirzepatide for laboratory research, Sempica Healthcare supplies independently tested research compounds to a 99.8% purity standard, with full Certificate of Analysis documentation available for each batch.
Research use only. Products sold on this website are intended for research purposes only. They are not for human consumption, medical use, or therapeutic application. By purchasing from this website, you confirm that you are a qualified professional and will use these products strictly for laboratory research.
[1] Pmc7526454 – https://pmc.ncbi.nlm.nih.gov/articles/PMC7526454/
[2] Pnas – https://www.pnas.org/doi/10.1073/pnas.2116506119
[4] Pmc9438179 – https://pmc.ncbi.nlm.nih.gov/articles/PMC9438179/
[5] insight.jci – https://insight.jci.org/articles/view/140532
[6] Full – https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2024.1431292/full
[7] Pmc12361993 – https://pmc.ncbi.nlm.nih.gov/articles/PMC12361993/
[8] Pmc7843845 – https://pmc.ncbi.nlm.nih.gov/articles/PMC7843845/
[9] Glp 1 Agonists The Latest Obesity Long Term Use Data – https://www.medcentral.com/endocrinology/obesity/glp-1-agonists-the-latest-obesity-long-term-use-data
[10] Nbk585056 – https://www.ncbi.nlm.nih.gov/books/NBK585056/
Semaglutide vs tirzepatide which is better for

Confused on Retatrutide vs Tirzepatide for weight
What is Tirzepatide dual GIP GLP-1 agonist