Semaglutide vs tirzepatide which is better for weight loss
Semaglutide vs tirzepatide which is better for
Quick Answer
Tirzepatide consistently outperforms semaglutide in head-to-head research for body weight reduction, with clinical trial data showing approximately 4 kg greater mean weight loss across studies and real-world cohort data confirming faster and deeper responses at six months [3][5]. Both compounds are GLP-1 receptor agonists, but tirzepatide’s additional GIP receptor activity appears to drive the performance difference. For type 2 diabetes glycaemic control, both compounds produce clinically meaningful HbA1c reductions, though tirzepatide again shows a modest but consistent advantage in comparative studies [10].
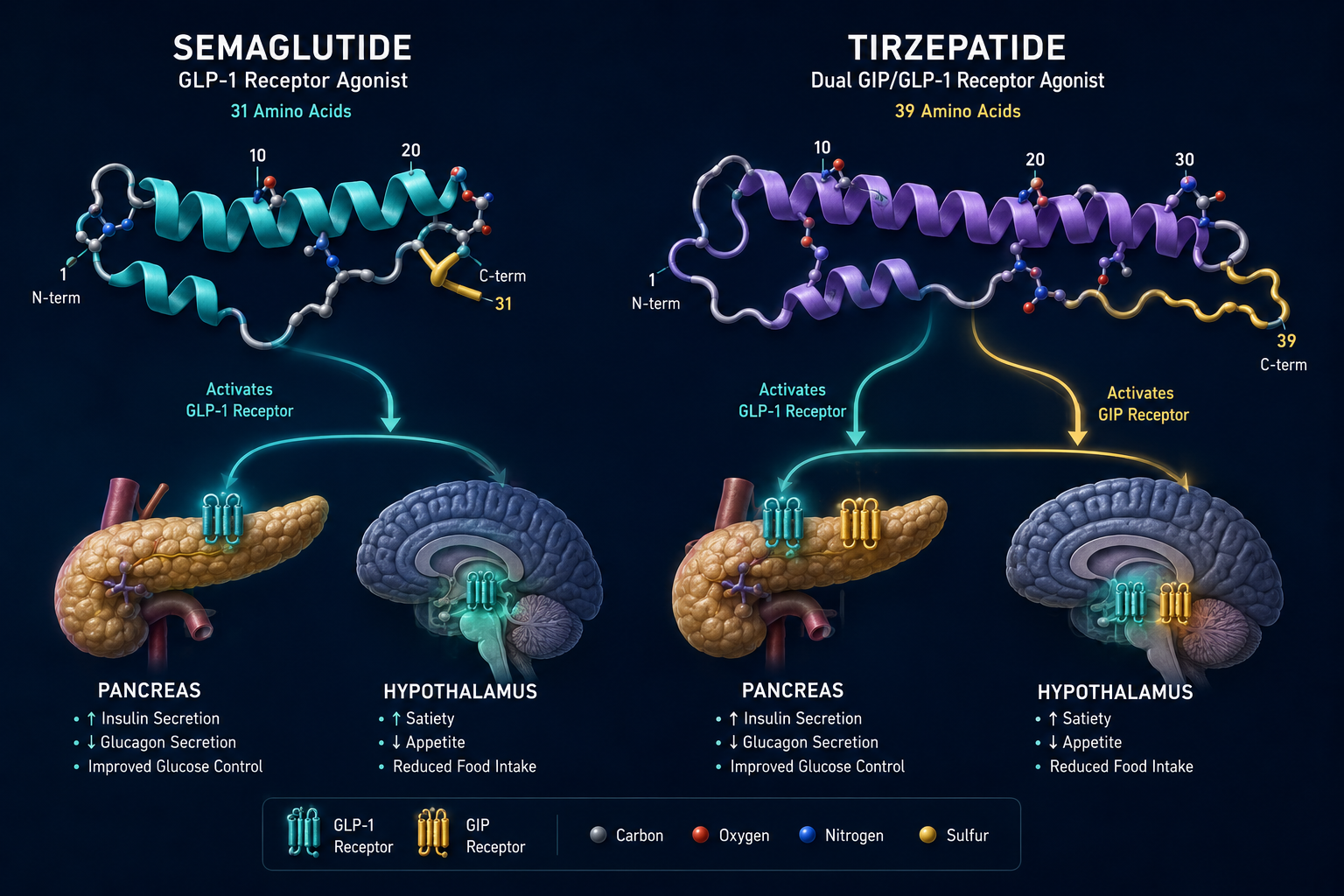
Semaglutide is a 31-amino-acid synthetic peptide classified as a GLP-1 (glucagon-like peptide-1) receptor agonist. Tirzepatide is a 39-amino-acid synthetic peptide that simultaneously activates both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors. This dual-agonist mechanism is the central distinction in any semaglutide vs tirzepatide research comparison.
Semaglutide’s mechanism centres on GLP-1 receptor activation across three primary sites:
Its acylated structure extends its half-life to approximately seven days, enabling once-weekly dosing in research protocols.
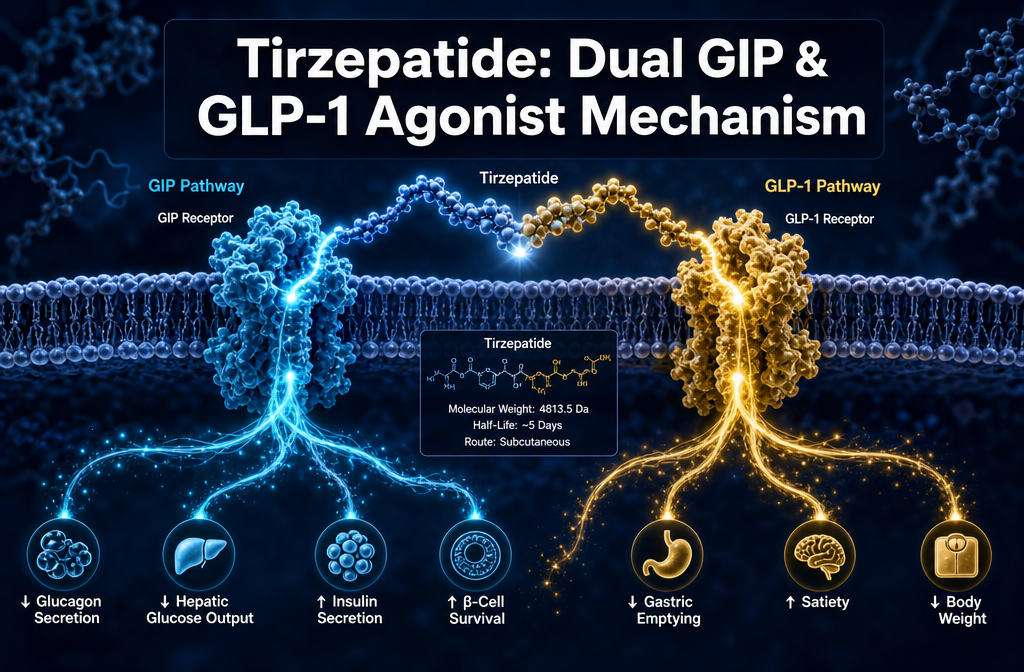
Tirzepatide’s mechanism builds on GLP-1 agonism and adds GIP receptor activation. GIP receptors are expressed in adipose tissue, bone, and the brain, and their co-stimulation appears to produce additive effects on insulin secretion, fat metabolism, and appetite suppression beyond what GLP-1 agonism alone achieves. Tirzepatide carries a C20 fatty diacid moiety that extends its half-life to approximately five days.
Research framing note: In laboratory investigations, both compounds are studied as lyophilised peptide powders requiring reconstitution with bacteriostatic water prior to use. Researchers sourcing these compounds for metabolic pathway studies can find GLP-1/GIP multi-pathway metabolic research peptides through Sempica’s dedicated research catalogue.
Tirzepatide produces greater weight loss than semaglutide in both randomised controlled trials and real-world research populations. This is the most consistently replicated finding across the current body of evidence.
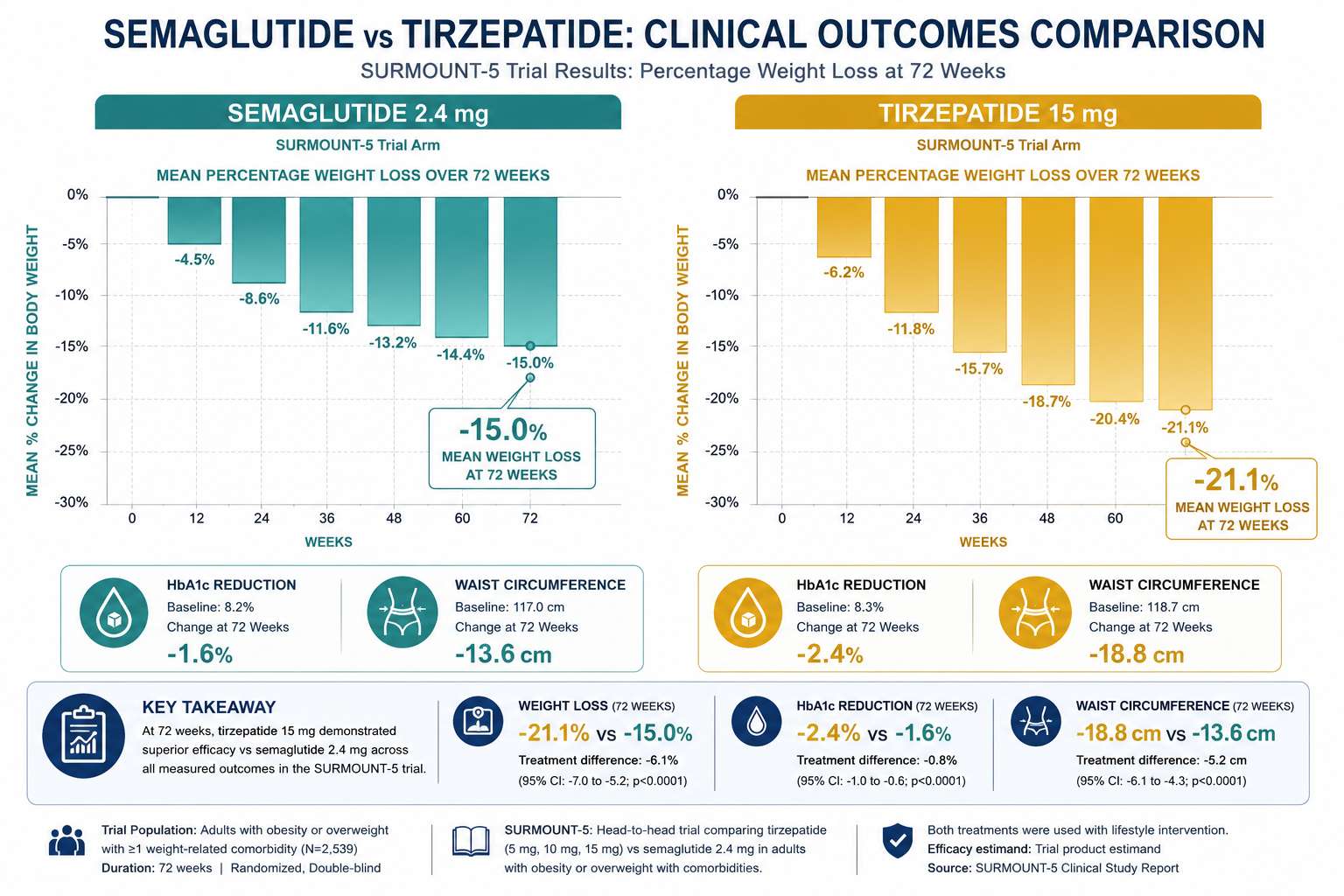
The SURMOUNT-5 trial, published in the New England Journal of Medicine, provided the most direct head-to-head comparison to date. Over 72 weeks, participants assigned to tirzepatide achieved significantly greater percentage body weight reduction and waist circumference reduction compared to those receiving semaglutide [5]. This was a randomised design, which limits confounding and makes it the strongest single data point in the semaglutide vs tirzepatide research comparison.
A large real-world cohort study analysed through the Truveta platform found approximately 11% body weight reduction with tirzepatide versus approximately 9% with semaglutide at the six-month mark [7]. A separate meta-analysis pooling data across multiple studies estimated tirzepatide’s advantage at approximately 4 kg of additional weight loss compared to semaglutide [4].
How quickly do patients see results with each compound?
Real-world data suggest tirzepatide produces measurable weight reduction faster than semaglutide. The Truveta cohort study found tirzepatide-treated subjects reached clinically meaningful thresholds sooner than semaglutide-treated subjects, though both compounds showed progressive weight reduction over time [7]. In research models, the onset of appetite-suppressing effects is typically observed within the first few weeks of exposure to either compound.
| Metric | Semaglutide | Tirzepatide |
|---|---|---|
| Receptor targets | GLP-1 | GLP-1 + GIP |
| Amino acids | 31 | 39 |
| Half-life | ~7 days | ~5 days |
| Mean weight loss (real-world, 6 months) | ~9% [7] | ~11% [7] |
| Advantage over comparator (meta-analysis) | Reference | ~4 kg greater [4] |
| SURMOUNT-5 outcome | Comparator | Superior [5] |
Both compounds produce substantial HbA1c reductions in type 2 diabetes research models, but tirzepatide demonstrates a consistent, modest advantage in glycaemic outcomes. A comparative effectiveness study published in Diabetes Care found tirzepatide superior to semaglutide for HbA1c reduction in a real-world population of adults with type 2 diabetes [10].
Semaglutide’s GLP-1 mechanism drives glucose-dependent insulin secretion and glucagon suppression, both well-established pathways in diabetes research. Tirzepatide adds GIP receptor activation, which contributes additional insulin-sensitising effects, particularly in adipose tissue — a distinction that may explain the incremental glycaemic benefit observed in comparative research [2].
For researchers investigating insulin resistance models and metabolic pathway interactions, Sempica’s metabolic and energy research compounds catalogue covers both compounds alongside related agents such as MOTS-c, which modulates AMPK signalling and insulin sensitivity through a distinct mitochondrial pathway.
Both compounds share a broadly similar gastrointestinal side-effect profile. Nausea, vomiting, diarrhoea, and constipation are the most frequently reported adverse events in clinical research populations, and these are generally dose-dependent and transient.
Common adverse events reported in clinical trials:
Which compound has fewer injection site reactions?
Published comparative data do not indicate a clinically meaningful difference in injection site reactions between the two compounds. Both are administered via subcutaneous injection in research protocols, and local tolerability appears broadly comparable across studies [4][5]. The American College of Cardiology’s review of comparative data notes that the side-effect profiles are similar enough that tolerability alone is unlikely to differentiate the compounds in most research contexts [2].
Are there serious adverse events to consider?
Preclinical research has identified potential associations with thyroid C-cell changes for GLP-1 receptor agonists as a class. Both compounds carry this class-level consideration in their research profiles. Pancreatitis has been reported as a rare adverse event in clinical populations. These findings are relevant context for laboratory investigators designing research protocols with either compound [1].
This question applies to clinical populations and is included here for research context. In clinical settings, both compounds are contraindicated in individuals with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2, due to the class-level GLP-1 receptor agonist risk profile. They are also not recommended during pregnancy.
For research purposes, these contraindication profiles are relevant when designing preclinical models and interpreting translational data. Researchers should account for these exclusion criteria when evaluating clinical trial populations in comparative studies.
Important: All Sempica research compounds are intended exclusively for laboratory research by qualified professionals. They are not for human consumption, medical use, or therapeutic application.
Tirzepatide is projected to deliver better health outcomes at a lower lifetime cost than semaglutide in obesity care modelling. A cost-effectiveness analysis published in 2026 found that tirzepatide’s superior weight loss outcomes, when modelled over a patient lifetime, offset its comparable acquisition cost and produced a favourable incremental cost-effectiveness ratio versus semaglutide [6].
In the U.S. market, both branded compounds (Ozempic/Wegovy for semaglutide; Mounjaro/Zepbound for tirzepatide) carry list prices in the range of several hundred to over one thousand U.S. dollars per month without insurance coverage, though actual costs vary significantly by payer, formulary, and geography. Cost remains a primary barrier to access in real-world obesity care, and this is an active area of health economics research [6][9].
For laboratory procurement of research-grade compounds, researchers should source from suppliers that provide independently verified Certificates of Analysis (CoA) confirming purity and potency. Sempica maintains a 99.8% purity standard across its catalogue, with CoAs available for all compounds. Research-grade semaglutide (10mg) and tirzepatide (30mg) are available through Sempica’s digital storefront.
In clinical practice, switching from semaglutide to tirzepatide is done under medical supervision, typically with a washout or dose-adjustment period. In research models, the approach to compound switching depends on the study design, the endpoint being measured, and the half-life of each compound.
Given semaglutide’s approximately seven-day half-life and tirzepatide’s approximately five-day half-life, a minimum washout period of four to five half-lives (approximately four to five weeks) is standard practice when transitioning between agents in pharmacological research to avoid receptor saturation artefacts. Researchers designing crossover studies should account for this when planning timelines.
For laboratories exploring multi-pathway incretin research, Sempica also supplies tirzepatide (60mg) for higher-volume research protocols, as well as next-generation triple-agonist compounds such as retatrutide (40mg) for comparative metabolic studies.
Weight loss effects from both compounds are sustained during continued exposure in research populations, but weight regain following discontinuation is well-documented. A key finding across GLP-1 and dual-agonist research is that the appetite-suppressing and metabolic effects are dependent on ongoing receptor activation — they are not permanent structural changes.
Long-term cardiovascular outcomes data for semaglutide are more mature than for tirzepatide, given semaglutide’s earlier entry into clinical research. The SELECT trial demonstrated cardiovascular risk reduction with semaglutide in a high-risk obesity population, establishing an important precedent for GLP-1 agonist cardiovascular research. Tirzepatide’s long-term cardiovascular outcomes trial (SURPASS-CVOT) is ongoing, and its results will be a critical data point in the evolving semaglutide vs tirzepatide research comparison [2][8].
Regarding long-term safety, the most actively monitored signals in ongoing research include thyroid C-cell effects, pancreatic safety, and potential muscle mass loss alongside fat mass reduction — the latter being particularly relevant for body composition research models.
The choice between semaglutide and tirzepatide in a research context depends on the specific pathway being investigated. Tirzepatide is the preferred compound when the research question involves maximal body weight reduction, dual incretin receptor pharmacology, or GIP receptor biology. Semaglutide is appropriate when the research focuses specifically on isolated GLP-1 receptor agonism, cardiovascular outcomes (where the evidence base is more established), or when a well-characterised reference compound is needed for comparison.
For researchers exploring the frontier of incretin-based metabolic research, the triple-agonist retatrutide (GLP-1/GIP/glucagon) represents the next comparison point beyond tirzepatide. Sempica’s GLP-1/GIP multi-pathway metabolic research peptides page provides a structured overview of compounds across this receptor class.
Researchers interested in adjacent metabolic pathways — such as visceral fat reduction via growth hormone-releasing mechanisms — may also find value in reviewing tesamorelin research for visceral fat and endocrine metabolic studies, which operates through a distinct GH-axis mechanism.
Q: What is the primary structural difference between semaglutide and tirzepatide?
Semaglutide is a 31-amino-acid GLP-1 receptor agonist. Tirzepatide is a 39-amino-acid dual GIP/GLP-1 receptor agonist with a C20 fatty diacid moiety. The additional GIP receptor activity is the key pharmacological distinction.
Q: Which compound produces greater weight loss in clinical research?
Tirzepatide consistently produces greater weight loss than semaglutide across randomised trials and real-world cohort studies, with approximately 4 kg greater mean weight loss in meta-analyses and superior outcomes in the SURMOUNT-5 head-to-head trial [4][5].
Q: Are the side-effect profiles different between the two compounds?
Both compounds share a similar gastrointestinal side-effect profile dominated by nausea, vomiting, and diarrhoea. Injection site reactions appear comparable. There is no strong evidence that one compound is meaningfully better tolerated than the other [2][4].
Q: Which compound is more cost-effective?
Cost-effectiveness modelling published in 2026 projects tirzepatide to deliver better health outcomes at a lower lifetime cost than semaglutide in obesity care scenarios, driven by its superior weight loss efficacy [6].
Q: How do the half-lives of these compounds compare?
Semaglutide has a half-life of approximately seven days; tirzepatide has a half-life of approximately five days. Both support once-weekly dosing in research protocols.
Q: Is there long-term cardiovascular outcomes data for both compounds?
Long-term cardiovascular outcomes data are more mature for semaglutide (SELECT trial). Tirzepatide’s cardiovascular outcomes trial (SURPASS-CVOT) is ongoing as of 2026 [2][8].
Q: What is the correct storage protocol for these research compounds?
Both compounds should be stored as lyophilised powder at -20°C. Reconstituted solutions should be refrigerated at 2–8°C and used within 28 days. Never freeze a reconstituted solution.
Q: Where can qualified researchers source these compounds?
Sempica supplies both semaglutide and tirzepatide as research-grade lyophilised compounds, independently tested to 99.8% purity, with Certificates of Analysis available. See the Sempica research compound guide for procurement guidance.
Q: Are these compounds appropriate for human use?
No. All Sempica research compounds are strictly for laboratory research by qualified professionals. They are not for human consumption, medical use, or therapeutic application.
Q: What comes after tirzepatide in incretin research?
Retatrutide, a triple GLP-1/GIP/glucagon receptor agonist, is the next compound in this research lineage and is currently being studied in direct comparison with both tirzepatide and semaglutide.
The semaglutide vs tirzepatide research comparison has produced a clear and consistent picture across randomised trials, real-world cohort studies, and meta-analyses: tirzepatide’s dual GIP/GLP-1 receptor mechanism delivers greater weight reduction and comparable or superior glycaemic outcomes relative to semaglutide’s single-receptor approach [3][5][7]. The SURMOUNT-5 trial provides the most rigorous head-to-head evidence, and cost-effectiveness modelling now supports tirzepatide as the more efficient option in obesity research contexts [6].
For research professionals, the practical implications are clear. When designing metabolic research protocols that require maximal body weight or adiposity reduction, tirzepatide is the stronger research tool. When the research question specifically concerns isolated GLP-1 receptor pharmacology or requires a compound with a more established long-term cardiovascular evidence base, semaglutide remains a well-validated reference agent.
Actionable next steps for research professionals:
[1] jocmr.elmerjournals – https://jocmr.elmerjournals.com/jocmr/article/view/6231
[2] Semaglutide Vs Tirzepatide – https://www.acc.org/latest-in-cardiology/journal-scans/2024/07/15/14/37/semaglutide-vs-tirzepatide
[3] jamanetwork – https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2821080
[4] Pmc11231910 – https://pmc.ncbi.nlm.nih.gov/articles/PMC11231910/
[5] Nejmoa2416394 – https://www.nejm.org/doi/abs/10.1056/NEJMoa2416394
[6] Tirzepatide Vs Semaglutide Study Compares Cost And Health Outcomes In Obesity – https://www.news-medical.net/news/20260422/Tirzepatide-vs-semaglutide-Study-compares-cost-and-health-outcomes-in-obesity.aspx
[7] Tirzepatide Vs Semaglutide Real World Obesity Study – https://www.truveta.com/blog/research/tirzepatide-vs-semaglutide-real-world-obesity-study/
[8] Semaglutide Versus Tirzepatide For Weight Loss In Adults With Overweight Or Obesity – https://falkfoundation.org/en/fgr/detail/semaglutide-versus-tirzepatide-for-weight-loss-in-adults-with-overweight-or-obesity/
[9] S1871403x26000190 – https://www.sciencedirect.com/science/article/abs/pii/S1871403X26000190
[10] Comparative Effectiveness Of Tirzepatide Versus – https://diabetesjournals.org/care/article/49/5/808/164532/Comparative-Effectiveness-of-Tirzepatide-Versus
Research Use Only Disclaimer: All products referenced in this article are intended for research purposes only. They are not for human consumption, medical use, or therapeutic application. By purchasing from sempicahealthcare.ch, you confirm that you are a qualified professional and will use these products strictly for laboratory research.
Semaglutide vs tirzepatide which is better for

Confused on Retatrutide vs Tirzepatide for weight
What is Tirzepatide dual GIP GLP-1 agonist