
How to calculate peptide dosage for peptide
Unsure of How much of Ozempic of
Quick Answer
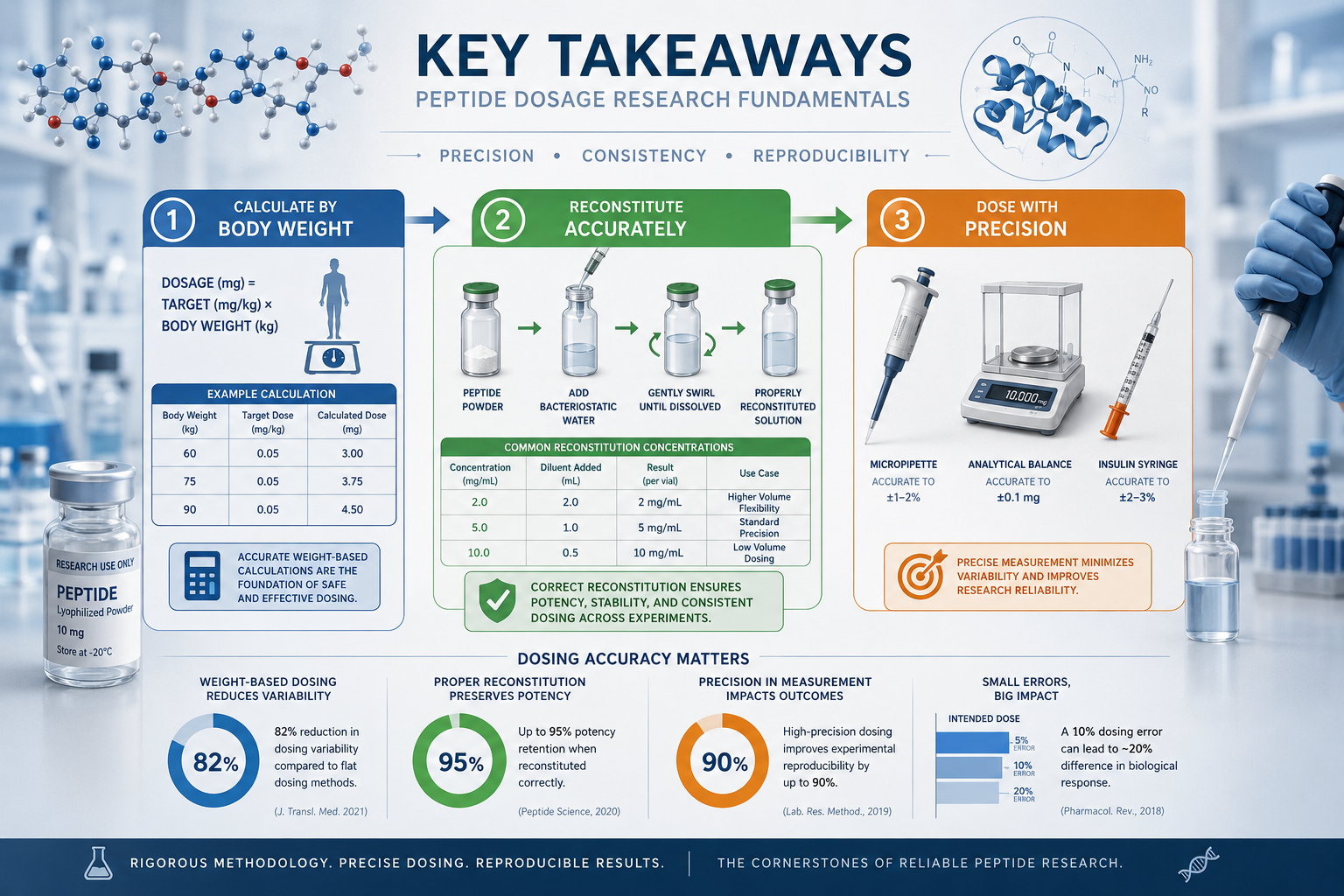
Calculating peptide dosage for research requires three core values: the total peptide amount in your vial (in milligrams), the volume of bacteriostatic water used for reconstitution (in millilitres), and the target dose per administration (in micrograms). The concentration after reconstitution determines how much volume you draw into the syringe to deliver the precise dose. For weight-based protocols, multiply the subject’s body mass by the specified mcg/kg dose, then convert that total into a draw volume using your reconstituted concentration.

Peptide dosage calculation in research settings depends entirely on the experimental protocol design. Weight-based dosing expresses the dose as micrograms per kilogram of body mass (mcg/kg), which scales the amount administered according to the subject’s size. Fixed-amount dosing delivers the same absolute dose to all subjects regardless of body mass, typically expressed as a set number of micrograms or milligrams per administration.
Weight-based protocols are standard when investigating dose-response relationships, pharmacokinetic profiles, or when translating findings across species with different body masses. For example, a protocol specifying 5 mcg/kg for a 78 kg subject would require 390 mcg per dose (5 × 78 = 390).[1] This approach normalises exposure across subjects of varying sizes and is particularly important for compounds with narrow therapeutic windows or when comparing results with published literature that uses weight-normalised dosing.
Fixed-amount dosing is appropriate when the research question focuses on absolute concentration effects, when all subjects fall within a narrow weight range, or when the protocol aims to replicate a specific previous study that used fixed dosing. Many metabolic research peptides use fixed dosing in controlled laboratory settings where subject weights are standardised.
When to choose weight-based dosing:
When to choose fixed-amount dosing:
Body surface area (BSA) normalisation offers a third approach for peptides with narrow therapeutic indices, providing more accurate scaling than simple weight-based calculations by accounting for metabolic rate differences.[2] BSA-based dosing is less common in routine research but may be specified in advanced protocols.
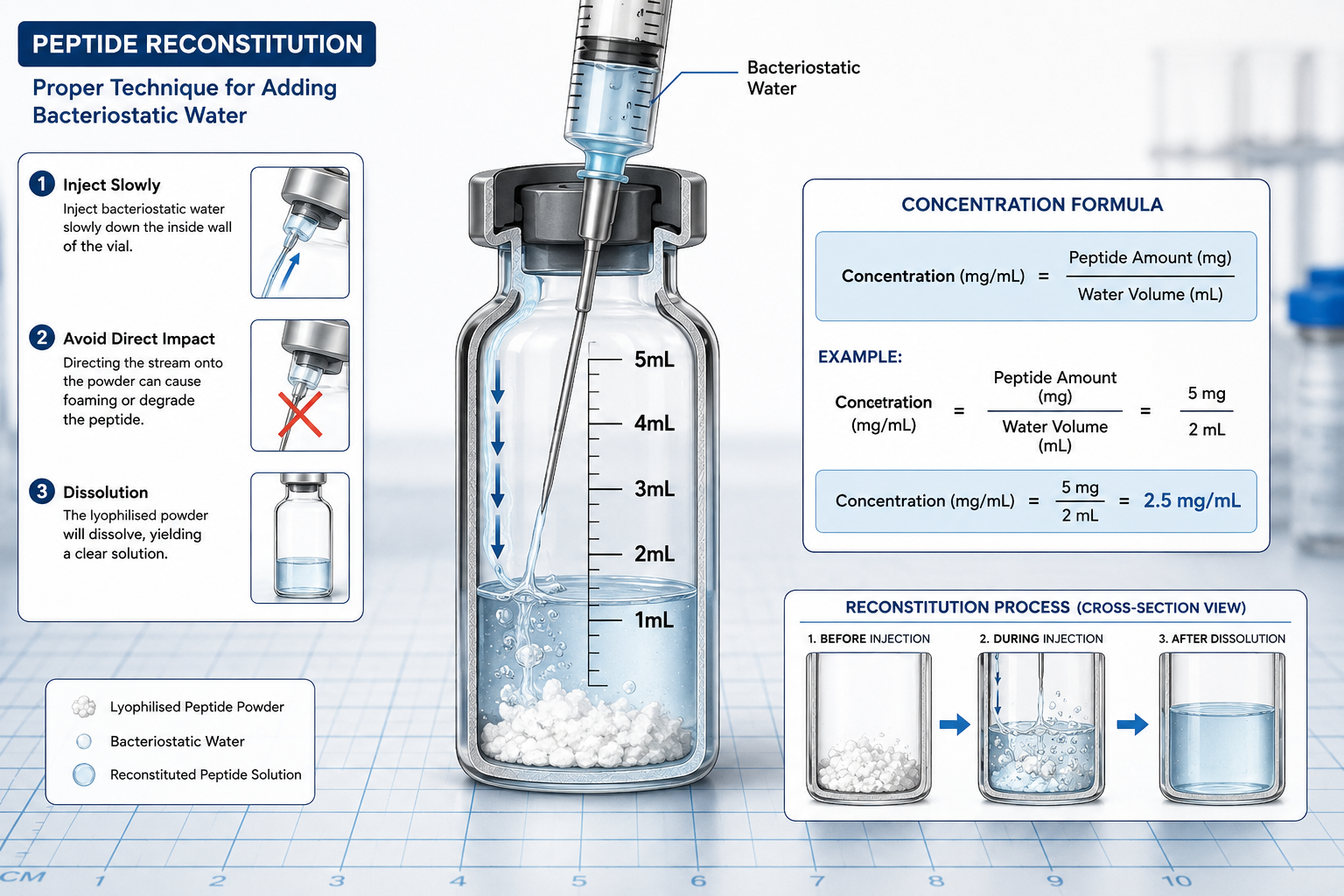
Reconstitution transforms lyophilised peptide powder into a liquid solution with a known concentration, which is the foundation for all subsequent dosing calculations. The process requires bacteriostatic water (0.9% benzyl alcohol), sterile technique, and careful attention to the final volume to ensure accurate concentration.
Standard reconstitution protocol:
The volume of bacteriostatic water you add determines the final concentration. A 5 mg vial reconstituted with 1 mL yields 5 mg/mL, while the same vial reconstituted with 3 mL yields approximately 1.7 mg/mL.[3] Neither approach changes the total amount of peptide—only the concentration and therefore the volume you must draw for each dose.
Bacteriostatic water is the standard diluent because the benzyl alcohol preservative prevents bacterial growth, extending the usable life of the reconstituted solution to 14 days when refrigerated at 2–8°C. Sterile water contains no preservative and should only be used for single-use applications where the entire vial will be consumed within 24 hours. For detailed reconstitution protocols, refer to our comprehensive laboratory guide on mixing and storing peptides.
Common reconstitution mistakes to avoid:
The fundamental calculation for peptide dosing converts the known peptide amount and dilution volume into a concentration, then determines the draw volume needed to deliver the target dose. The formula is straightforward: Concentration (mg/mL) = Total peptide amount (mg) ÷ Dilution volume (mL).
Once you know the concentration, you can calculate the volume needed for any specific dose: Draw volume (mL) = Target dose (mg) ÷ Concentration (mg/mL). Because most research doses are expressed in micrograms (mcg) rather than milligrams (mg), you must convert units: 1 mg = 1,000 mcg.
Worked example:
You have a 5 mg vial of BPC-157 and reconstitute it with 2 mL of bacteriostatic water.
On a standard U-100 insulin syringe, 0.1 mL equals 10 units.
International Units (IU) are used for some peptides and proteins where biological activity rather than mass determines dosing. Growth hormone, for instance, is commonly dosed in IU. The conversion between mg and IU is compound-specific and must be provided by the manufacturer or protocol documentation. For somatropin (recombinant human growth hormone), the standard conversion is approximately 3 IU per 1 mg, but this varies by formulation and must never be assumed.[4]
Quick reference conversions:
Several online peptide dosage calculators automate these conversions. These tools typically ask for peptide amount (mg), dilution volume (mL), and target dose (mcg), then output the required draw volume in both millilitres and syringe units.[4][6] While calculators reduce arithmetic errors, understanding the underlying mathematics ensures you can verify results and troubleshoot discrepancies.
For cycle planning, estimate total peptide needed by multiplying daily dose by the number of days: Total peptide (mg) = Daily dose (mcg) × Cycle days ÷ 1,000.[1] A 30-day cycle at 250 mcg per day requires 7.5 mg total (250 × 30 ÷ 1,000 = 7.5).
Research peptide dosing prioritises experimental consistency, protocol adherence, and data reproducibility. Therapeutic dosing in clinical settings optimises for patient outcomes, safety monitoring, and individualised dose titration. These fundamentally different objectives lead to distinct approaches in dose selection, adjustment, and administration.
Research protocols typically specify exact doses, fixed administration schedules, and standardised subject characteristics to minimise variability and enable comparison across studies. A research protocol might call for 5 mcg/kg administered subcutaneously once daily at 09:00 hours for 28 consecutive days, with no provision for dose adjustment based on individual response. This rigidity is essential for generating reproducible data and isolating the effects of the compound from confounding variables.
Therapeutic dosing, by contrast, begins with an initial dose and adjusts based on individual response, tolerability, adverse effects, and clinical endpoints. A clinician might start a patient at 25% of the target dose and titrate upward over several weeks while monitoring biomarkers and symptoms.[2] This individualised approach optimises benefit-risk balance for each patient but introduces variability that would confound research data.
Key distinctions:
| Aspect | Research Dosing | Therapeutic Dosing |
|---|---|---|
| Primary goal | Data reproducibility | Patient outcome optimisation |
| Dose adjustment | Fixed per protocol | Individualised titration |
| Subject selection | Standardised characteristics | Heterogeneous patient populations |
| Administration timing | Rigidly scheduled | Flexible within guidelines |
| Monitoring focus | Protocol compliance | Safety and efficacy endpoints |
| Documentation | Detailed for regulatory review | Clinical notes and EMR |
Research dosing also differs in the range of doses investigated. Preclinical studies often include doses far exceeding any anticipated therapeutic use to establish toxicity thresholds and maximum tolerated doses. A dose-ranging study might test 1, 10, 100, and 1,000 mcg/kg to map the full dose-response curve, even though only the lowest doses would ever be considered for therapeutic application.
The regulatory context differs as well. Research use of peptides falls under laboratory research exemptions and institutional review protocols, while therapeutic use requires regulatory approval, prescription oversight, and post-market surveillance. All Sempica compounds are supplied strictly for research purposes and carry the mandatory disclaimer: Products sold on this website are intended for research purposes only. They are not for human consumption, medical use, or therapeutic application.
The most frequent error in peptide reconstitution is confusing the volume of water added with the final volume of solution. When you add 2 mL of water to a lyophilised peptide, the final volume is slightly more than 2 mL because the peptide powder occupies space. For most peptides at research concentrations, this difference is negligible (typically less than 1%), but for large peptides or high concentrations, it can affect accuracy.
Mistake 1: Failing to account for stated purity
Peptide vials list the total mass of lyophilised material, which includes the active peptide plus any counter-ions, residual salts, or lyoprotectants. A vial labelled “5 mg” at 98% purity contains 4.9 mg of active peptide (5 × 0.98 = 4.9). For high-precision work, use the purity-adjusted amount in your concentration calculation: Adjusted peptide amount = Stated amount × (Purity % ÷ 100). Sempica compounds are manufactured to 99.8% purity, minimising this correction but not eliminating it entirely.
Mistake 2: Unit confusion between mg and mcg
Mixing up milligrams and micrograms leads to 1,000-fold dosing errors. Always write out units explicitly in your calculations and double-check conversions. A 250 mcg dose is 0.25 mg, not 250 mg. Using dimensional analysis helps prevent errors: (250 mcg) × (1 mg / 1,000 mcg) = 0.25 mg.
Mistake 3: Incorrect syringe unit interpretation
Standard insulin syringes are marked in units, not millilitres. A U-100 syringe has 100 units per 1 mL, so each unit equals 0.01 mL. A 0.15 mL draw volume equals 15 units on a U-100 syringe.[3] Using a U-40 syringe (40 units per mL) with calculations based on U-100 markings introduces a 2.5-fold error.
Mistake 4: Neglecting dead volume
Syringes and needles retain a small volume of solution (dead volume) that never gets injected. For standard insulin syringes with attached needles, dead volume is approximately 5–10 microlitres. This is usually negligible for doses above 50 mcg but can introduce 10–20% error for very small doses. Protocols requiring extreme precision may specify drawing slightly more than the calculated volume to compensate.
Mistake 5: Assuming all peptides reconstitute to the same concentration
Different peptides have different molecular weights and solubility characteristics. A 5 mg vial of a small peptide like Epithalon (molecular weight ~390 Da) occupies less volume than 5 mg of a large peptide like semaglutide (molecular weight ~4,100 Da). While this rarely affects practical reconstitution at typical research concentrations, it matters for high-concentration formulations or when working near solubility limits.
Mistake 6: Using the wrong diluent
Some peptides require specific reconstitution buffers rather than plain bacteriostatic water. Copper peptides like GHK-Cu may require slightly acidic conditions, while some acetate salts dissolve better in sterile water. Always verify the recommended diluent in the product documentation or research compound specifications.
Insulin syringes are the standard tool for peptide administration in research settings because they provide precise measurement in small volumes (0.3–1.0 mL) and are designed for subcutaneous injection. Accurate measurement requires understanding syringe markings, proper drawing technique, and awareness of measurement limitations.
Understanding U-100 syringe markings:
U-100 insulin syringes are calibrated for 100 units per millilitre. Each small line typically represents 1 unit (0.01 mL), and each large line represents 5 or 10 units depending on syringe size. A 0.5 mL (50-unit) syringe has markings every 1 unit up to 50 units. A 1.0 mL (100-unit) syringe extends to 100 units.
To convert your calculated draw volume in millilitres to syringe units: Units = Volume (mL) × 100. A draw volume of 0.08 mL equals 8 units (0.08 × 100 = 8).
Proper drawing technique:
Measurement precision and limitations:
Insulin syringes provide accuracy within ±5% for volumes above 0.1 mL (10 units) when used correctly. Below 0.05 mL (5 units), measurement error increases significantly due to the relative size of the meniscus and the difficulty of reading small volumes precisely. For doses requiring less than 5 units, consider reconstituting to a lower concentration so the draw volume increases into the more accurate range.
Reading the meniscus:
The liquid surface in the syringe forms a slight curve (meniscus). Always read the measurement at the bottom of the meniscus at eye level. Reading from above or below introduces parallax error. For clear solutions, the bottom of the meniscus should align with the target marking. For opaque or coloured solutions, align the centre of the liquid column.
Syringe selection for different dose ranges:
For research requiring doses below 5 units, consider using a 0.3 mL syringe with half-unit markings (if available) or reconstituting to a lower concentration. For example, if your calculation yields 3 units (0.03 mL), reconstituting with twice the water volume would double the draw volume to 6 units (0.06 mL), improving measurement accuracy.
Target concentration depends on three factors: the dose range specified in your protocol, the practical limits of accurate syringe measurement, and the solubility characteristics of the specific peptide. The goal is to choose a concentration that places your typical draw volume in the 0.1–0.5 mL range (10–50 units on a U-100 syringe), where measurement accuracy is highest.
General concentration guidelines:
For most research peptides administered in the 100–500 mcg dose range, reconstituting to 1–3 mg/mL provides practical draw volumes. A 250 mcg dose from a 2 mg/mL solution requires 0.125 mL (12.5 units)—well within the accurate measurement range.
For peptides dosed in the microgram range (10–100 mcg), lower concentrations of 0.5–1 mg/mL prevent draw volumes from becoming impractically small. A 50 mcg dose from a 0.5 mg/mL solution requires 0.1 mL (10 units), which is at the lower limit of accurate measurement but still workable.
For peptides dosed in the milligram range (1–10 mg), higher concentrations of 5–10 mg/mL keep draw volumes manageable. A 5 mg dose from a 10 mg/mL solution requires 0.5 mL (50 units), which is convenient and accurate.
Worked example for concentration selection:
You have a 10 mg vial of TB-500 and your protocol calls for 2 mg per dose, twice weekly.
Option 1 provides the best balance: the draw volume is large enough for accurate measurement but small enough to be practical for subcutaneous injection. Option 2 requires the full capacity of a 1 mL syringe, leaving no margin for error. Option 3 works but offers less measurement precision at the lower volume.
Solubility considerations:
Most synthetic peptides are highly soluble in bacteriostatic water at concentrations up to 10 mg/mL. Some peptides, particularly those with high hydrophobicity or specific structural features, may have lower solubility limits. If a peptide does not fully dissolve after gentle swirling for 2–3 minutes, the concentration may exceed its solubility limit. In this case, add more bacteriostatic water in 0.5 mL increments until complete dissolution occurs, then recalculate your concentration.
Copper peptides like GHK-Cu may require slightly acidic conditions (pH 5–6) for optimal solubility. If using plain bacteriostatic water results in incomplete dissolution, consult the product documentation for recommended reconstitution buffers.
Storage stability and concentration:
Higher concentrations generally show better stability during refrigerated storage because there is less water available for hydrolysis reactions. However, this advantage is minor compared to proper temperature control (2–8°C) and protection from light. For most research applications, choose concentration based on dosing convenience rather than storage considerations, as properly stored reconstituted peptides remain stable for 14 days regardless of concentration within the typical range.
Rodent models require species-specific dose calculations because mice and rats differ substantially in body mass, metabolic rate, and pharmacokinetic parameters. A dose that produces a specific effect in mice will not produce the same effect in rats when scaled by body weight alone, due to allometric scaling principles.
Body weight scaling:
The simplest approach multiplies the mcg/kg dose by the animal’s body weight. A 25-gram mouse receiving 5 mcg/kg would get 125 mcg per dose (0.025 kg × 5 mcg/kg = 0.125 mg = 125 mcg). A 250-gram rat at the same mcg/kg dose would receive 1,250 mcg (0.250 kg × 5 mcg/kg = 1.25 mg = 1,250 mcg).[1]
This approach assumes linear scaling, which is acceptable for initial dose-finding studies but may not account for metabolic rate differences. Smaller animals have higher mass-specific metabolic rates, meaning they clear drugs faster and may require higher mcg/kg doses to achieve equivalent exposure.
Allometric scaling for cross-species translation:
Allometric scaling adjusts doses based on body surface area or metabolic rate rather than simple body weight. The formula uses an exponent less than 1.0 to account for the non-linear relationship between body size and metabolic rate. A common approach uses the 0.75 power of body weight: Dose₂ = Dose₁ × (Weight₂ / Weight₁)^0.75.
To translate a mouse dose to a rat dose using allometric scaling:
The allometrically scaled rat dose (2.8 mg/kg) is lower than the simple weight-scaled dose (5 mg/kg), reflecting the rat’s lower mass-specific metabolic rate.
Practical considerations for rodent dosing:
Injection volume limits differ between species. Mice tolerate subcutaneous injections up to 0.1 mL per site (maximum 0.2 mL total if using two sites). Rats tolerate up to 0.5 mL per subcutaneous site. These volume limits may constrain your concentration choices. If your calculated dose for a mouse requires 0.15 mL, you must either increase concentration or split the dose across two injection sites.
Species-specific pharmacokinetics:
Some peptides show markedly different half-lives or bioavailability between mice and rats due to differences in peptidase activity, renal clearance, or receptor expression. When translating protocols between species, consult published pharmacokinetic data for the specific peptide when available. Compounds like MOTS-c may require species-specific dose optimisation based on preliminary studies.
Standard research doses for common peptides:
| Peptide | Mouse Dose (mcg/kg) | Rat Dose (mcg/kg) | Notes |
|---|---|---|---|
| BPC-157 | 10–500 | 10–500 | Linear scaling typical |
| TB-500 | 5–20 mg/kg | 5–20 mg/kg | Dosed in mg range |
| Semaglutide | 10–100 | 10–100 | GLP-1 agonist |
| Epithalon | 1–10 | 1–10 | Telomerase activator |
These ranges are illustrative; actual doses depend on the specific research question, administration route, and study design.
Peptide purity represents the percentage of the lyophilised material that consists of the active peptide sequence, with the remainder comprising counter-ions (typically acetate or trifluoroacetate), residual salts from synthesis, moisture, and lyoprotectants. Adjusting for purity ensures you deliver the intended amount of active peptide rather than total lyophilised mass.
Purity adjustment formula:
Active peptide amount (mg) = Stated amount (mg) × (Purity % ÷ 100)
A 5 mg vial at 95% purity contains 4.75 mg of active peptide (5 × 0.95 = 4.75). If your protocol specifies 250 mcg of active peptide per dose, you must account for this difference in your concentration calculation.
When purity adjustment matters:
For peptides at 98% purity or higher—such as all Sempica compounds manufactured to 99.8% purity—the adjustment is minimal (0.2% difference) and often omitted in routine research. The error introduced by neglecting a 0.2% purity correction is smaller than the measurement error of most laboratory balances and syringes.
For peptides below 95% purity, adjustment becomes important for dose-response studies, pharmacokinetic investigations, or any research requiring high precision. A peptide at 85% purity requires an 18% increase in the amount of lyophilised material used to deliver the same active peptide dose as a 99% pure compound.
Worked example with purity adjustment:
Your protocol requires 500 mcg of active BPC-157 per dose. You have a 5 mg vial stated at 92% purity.
Without purity adjustment, you would have calculated 2.5 mg/mL concentration and drawn 20 units, delivering only 460 mcg of active peptide—an 8% underdose.
Certificate of Analysis (CoA) verification:
Reputable suppliers provide Certificates of Analysis documenting purity via HPLC (high-performance liquid chromatography) or mass spectrometry. The CoA should specify purity as a percentage and identify major impurities. Sempica provides CoAs for all compounds, ensuring transparency and enabling accurate dose calculations.
Purity versus potency:
Purity measures the proportion of active peptide in the lyophilised material. Potency measures the biological activity of that peptide compared to a reference standard. A peptide can be 99% pure but have reduced potency if the peptide structure has degraded or if the specific sequence has lower-than-expected receptor binding. For most synthetic peptides used in research, purity and potency correlate closely, but for complex proteins or peptides with critical post-translational modifications, potency testing may be necessary.
Administration route significantly affects peptide pharmacokinetics, bioavailability, and therefore effective dosing. Subcutaneous (SC) and intravenous (IV) routes differ in absorption kinetics, peak concentration, and duration of exposure, requiring route-specific dose adjustments in many protocols.
Bioavailability differences:
Intravenous administration delivers 100% of the dose directly into systemic circulation, achieving immediate peak plasma concentration. Subcutaneous administration requires absorption from the injection depot through capillaries and lymphatics, resulting in lower bioavailability (typically 50–90% depending on the peptide) and delayed peak concentration (30 minutes to 2 hours post-injection).
For peptides with high subcutaneous bioavailability (above 80%), the dose difference between routes may be minimal. For peptides with lower bioavailability or significant first-pass metabolism, the subcutaneous dose must be increased to achieve equivalent systemic exposure to an IV dose.
Absorption kinetics and dosing frequency:
Subcutaneous injection creates a depot that releases peptide gradually, extending the duration of exposure and potentially allowing less frequent dosing. A peptide with a 4-hour half-life might require IV dosing every 4–6 hours to maintain steady-state levels, while subcutaneous dosing every 8–12 hours could achieve similar average exposure due to the sustained absorption phase.
Conversely, IV administration provides precise control over plasma concentration and is preferred when rapid onset is required or when investigating acute pharmacodynamic effects. Dose-response studies often use IV administration to eliminate absorption variability as a confounding factor.
Route-specific dose adjustment guidelines:
When translating a protocol from IV to SC administration, a common starting point is to increase the dose by 20–50% to compensate for incomplete bioavailability, then adjust based on measured outcomes. For example, an IV dose of 100 mcg might translate to an SC dose of 120–150 mcg.
When translating from SC to IV, reduce the dose by 20–40% and monitor closely, as the higher bioavailability and faster kinetics of IV administration increase the risk of exceeding the intended exposure.
Peptide-specific considerations:
Some peptides show minimal route-dependent differences. BPC-157 and TB-500, for instance, demonstrate robust activity via both SC and IV routes with similar effective dose ranges in published research. Other peptides, particularly those susceptible to peptidase degradation in subcutaneous tissue, may show substantially lower SC bioavailability.
GLP-1 receptor agonists like semaglutide are specifically engineered for subcutaneous administration with modifications (acylation, albumin binding) that extend half-life and improve bioavailability. These compounds are rarely administered IV in research settings because their pharmacokinetic profile is optimised for SC use.
Injection site effects:
Subcutaneous bioavailability can vary by injection site due to differences in blood flow and lymphatic drainage. Abdominal SC injections typically show faster absorption than injections in the thigh or flank. For protocols requiring high reproducibility, standardising the injection site across all subjects and time points is essential.
Volume and concentration constraints:
IV administration tolerates a wider range of concentrations because the solution is diluted immediately upon entering the bloodstream. SC administration is limited by the volume that can be comfortably injected at a single site (typically 0.5–1.0 mL in rats, 0.1 mL in mice) and by the osmolarity and pH of the solution, which must be compatible with subcutaneous tissue to avoid irritation or depot formation that impairs absorption.
Dosing errors compromise data validity, introduce confounding variables, and in severe cases may harm research subjects or require study termination. The consequences depend on the magnitude and direction of the error, the peptide’s therapeutic index, and the study design.
Underdosing consequences:
Administering less than the intended dose produces weaker-than-expected effects, potentially leading to false-negative results where a compound appears ineffective when it would have shown activity at the correct dose. In dose-response studies, underdosing shifts the entire curve, making it impossible to accurately determine EC50 (half-maximal effective concentration) or other pharmacological parameters.
Systematic underdosing across all subjects in a study may go undetected if there is no positive control or if the investigators do not verify actual delivered doses. This is particularly problematic in exploratory studies investigating novel compounds where expected effect sizes are unknown.
Overdosing consequences:
Administering more than the intended dose increases the risk of adverse effects, off-target activity, and receptor saturation that obscures dose-response relationships. For peptides with narrow therapeutic windows, even modest overdosing (20–50% above target) can produce toxicity or confounding physiological responses.
In competitive binding studies or receptor pharmacology research, overdosing can saturate receptors, making it impossible to distinguish between high-affinity and low-affinity interactions. In metabolic studies, excessive doses of compounds like GLP-1 agonists can produce nausea, reduced food intake, or other effects that confound the primary endpoints.
Detection and correction:
Dosing errors are often discovered when results deviate significantly from published literature using similar protocols, when dose-response curves show unexpected shapes, or during protocol audits. If an error is detected mid-study, the options are limited: continuing with the incorrect dose invalidates comparison with pre-error data, while correcting the dose creates a discontinuity in the dataset.
The best approach is prevention through systematic verification:
Regulatory and ethical implications:
In studies conducted under institutional animal care and use committee (IACUC) protocols, dosing errors may constitute protocol deviations requiring reporting and investigation. Significant errors that result in animal harm or compromise welfare may lead to protocol suspension.
For research intended to support regulatory submissions or publication in high-impact journals, dosing errors discovered after study completion may require study repetition or extensive additional validation to demonstrate that the error did not materially affect conclusions.
Common scenarios and their impact:
Dosing frequency depends on the peptide’s half-life, the duration of pharmacodynamic effect, and the specific research question. The goal is to maintain plasma concentrations or receptor occupancy within the target range throughout the study period.
Half-life as the primary determinant:
Peptides with half-lives under four hours typically require multiple daily doses (two to three times per day) to maintain steady-state levels. Peptides with half-lives exceeding eight hours can usually be dosed once daily. Peptides with half-lives in the 4–8 hour range may require twice-daily dosing depending on the acceptable fluctuation in plasma concentration.[2]
Examples by half-life category:
Pharmacodynamic versus pharmacokinetic considerations:
Some peptides produce effects that outlast their plasma half-life due to receptor internalisation, downstream signalling cascades, or tissue depot formation. BPC-157, for instance, has a short plasma half-life but produces tissue repair effects that persist for days after a single dose. In such cases, dosing frequency may be based on the duration of the desired effect rather than plasma kinetics.
Conversely, some peptides with long half-lives may require loading doses or more frequent initial dosing to rapidly achieve steady-state levels. Semaglutide protocols often use weekly dosing at a constant level, but the compound takes 4–5 weeks to reach steady state due to its long half-life.
Study design considerations:
Acute studies investigating immediate effects typically use single-dose administration timed to coincide with peak plasma concentration. Chronic studies investigating cumulative effects, adaptation, or long-term outcomes require sustained exposure via regular dosing throughout the study period.
Dose-response studies may use different dosing frequencies for different dose levels. Low doses might be administered once daily, while higher doses are split into twice-daily administration to avoid peak concentration-related adverse effects while achieving the same total daily dose.
Practical constraints:
Research facility schedules and staffing often constrain dosing frequency. Twice-daily dosing requires morning and evening administration (typically 12 hours apart), which may not align with standard laboratory hours. Three-times-daily dosing (every 8 hours) is particularly challenging and may require weekend staffing or automated dosing systems.
For peptides requiring frequent dosing, continuous infusion via osmotic minipumps offers an alternative that maintains steady plasma levels without repeated injections. This approach is common for peptides with very short half-lives or when investigating effects of constant versus pulsatile exposure.
Timing consistency:
Regardless of frequency, maintaining consistent timing between doses is critical for reproducibility. Circadian rhythms, feeding schedules, and other time-dependent physiological variables can interact with peptide effects. Dosing at the same time each day (within a 1-hour window) minimises this variability.
For peptides affecting metabolism or appetite, such as GLP-1 and GIP receptor agonists, timing relative to feeding can significantly affect outcomes. Protocols should specify whether dosing occurs before, with, or after meals, and maintain this relationship consistently.
Storage conditions directly affect peptide stability, which in turn determines the accuracy and consistency of dosing throughout a study. Improper storage leads to degradation, aggregation, or loss of potency, effectively reducing the delivered dose even when the correct volume is administered.
Standard storage protocol for reconstituted peptides:
Reconstituted peptides should be stored at 2–8°C (refrigerator temperature) immediately after reconstitution and kept refrigerated except during the brief period required for dose preparation. Most peptides reconstituted in bacteriostatic water remain stable for 14 days under these conditions. Never freeze reconstituted peptide solutions, as ice crystal formation can disrupt peptide structure and cause irreversible aggregation.
Protect vials from light by storing in the original packaging or wrapping in aluminium foil. Many peptides, particularly those containing tryptophan or tyrosine residues, are photosensitive and degrade when exposed to UV or bright visible light.
Temperature excursions and stability:
Brief temperature excursions (15–30 minutes at room temperature during dose preparation) have minimal impact on stability. Extended periods at room temperature (over 2 hours) accelerate degradation, particularly for peptides susceptible to oxidation or hydrolysis. If a vial is accidentally left at room temperature for several hours, the extent of degradation depends on the specific peptide but may range from 5–20% loss of potency.
Repeated temperature cycling (removing from refrigerator, warming to room temperature, returning to refrigerator) is more damaging than a single extended excursion because each cycle promotes aggregation and chemical degradation. Minimise cycling by preparing multiple doses at once when practical, or by keeping the vial refrigerated and drawing doses quickly.
Signs of degradation:
Visual inspection can detect some forms of degradation. Discard reconstituted peptide solutions that show:
Many forms of degradation are not visually apparent. Peptides stored beyond the recommended 14-day period may appear normal but have significantly reduced potency.
Impact on dosing accuracy:
Degradation effectively reduces the concentration of active peptide in the solution, leading to underdosing even when the correct volume is drawn. A 10% loss of potency means each dose delivers only 90% of the intended amount. Over a multi-week study, progressive degradation can introduce a time-dependent confound where early doses are higher than late doses.
To maintain dosing accuracy throughout a study:
Lyophilised (unreconstituted) storage:
Lyophilised peptides are significantly more stable than reconstituted solutions. Store unreconstituted vials at -20°C in a freezer, protected from moisture and light. Under these conditions, most peptides remain stable until the expiry date (typically 2–3 years from manufacture). Once removed from the freezer for reconstitution, do not return the lyophilised vial to frozen storage, as condensation during thawing can introduce moisture that degrades the peptide.
Peptide-specific stability considerations:
Some peptides have shorter stability windows after reconstitution. Copper peptides like GHK-Cu may show reduced stability beyond 7 days due to copper-catalysed oxidation. Growth hormone and other large proteins may aggregate more readily than small peptides. Always consult product-specific storage recommendations when available.
For detailed storage protocols across different peptide classes, refer to our comprehensive laboratory guide on mixing and storing peptides.
Accounting for degradation in dose calculations is generally not necessary when following proper storage protocols and using reconstituted peptides within the recommended 14-day window. However, for extended studies, high-precision work, or when using peptides with known stability issues, degradation correction may improve accuracy.
When degradation correction is unnecessary:
For routine research using high-purity peptides (above 98%) stored properly at 2–8°C and used within 14 days of reconstitution, degradation is typically less than 5% and falls within the normal variability of biological systems and measurement error. The added complexity of degradation correction provides no meaningful improvement in data quality.
When degradation correction is warranted:
Long-term studies extending beyond 14 days where preparing fresh vials every two weeks is impractical may benefit from degradation correction. Some research facilities use stability-indicating assays (HPLC or mass spectrometry) to measure actual peptide concentration at intervals throughout the study, then adjust dosing to maintain consistent delivered amounts.
Studies investigating subtle dose-response relationships or comparing effects across multiple time points may require degradation correction to avoid confounding time-dependent changes in effect with time-dependent changes in delivered dose.
Estimating degradation rates:
Published stability data for specific peptides can provide degradation rate estimates. For example, if literature reports 10% degradation over 30 days at 4°C, the daily degradation rate is approximately 0.33% per day. A dose prepared on day 1 delivers 100% of the intended amount, while the same volume drawn on day 15 delivers approximately 95% (100% – 14 days × 0.33%/day).
In the absence of published data, conservative estimates assume 1–2% degradation per week for most peptides stored properly. This translates to approximately 2–4% loss over a 14-day period, which is generally acceptable for most research applications.
Practical degradation correction approach:
Rather than adjusting calculations for degradation, the more practical approach is to prepare fresh vials at intervals that keep degradation below 5%. For a 28-day study, prepare two vials and switch to the fresh vial on day 15. For a 56-day study, prepare four vials and switch every 14 days. This approach maintains consistent potency without requiring complex calculations or stability testing.
Accelerated degradation scenarios:
Certain conditions accelerate degradation beyond normal rates:
If any of these conditions occur, discard the vial and prepare fresh solution rather than attempting to correct for accelerated degradation.
Analytical verification:
For critical studies or when degradation is suspected, analytical verification via HPLC provides definitive measurement of remaining active peptide. A sample of the reconstituted solution is analysed and compared to a fresh standard. If the measured concentration is 10% lower than expected, subsequent doses can be increased proportionally (draw 10% more volume) to deliver the intended amount of active peptide.
What is the difference between peptide concentration and dose?
Concentration is the amount of peptide per unit volume of solution (typically mg/mL), while dose is the total amount of active peptide administered in a single injection (typically mcg or mg). Concentration determines how much volume you must draw to deliver the target dose. A 2 mg/mL concentration requires 0.1 mL to deliver a 200 mcg dose, while a 1 mg/mL concentration requires 0.2 mL for the same dose.
Can I use sterile water instead of bacteriostatic water for reconstitution?
Sterile water can be used for single-use applications where the entire vial will be consumed within 24 hours. For multi-dose vials used over several days, bacteriostatic water is required because the benzyl alcohol preservative prevents bacterial growth. Using sterile water for multi-dose applications creates contamination risk and requires discarding the vial after 24 hours.
How do I convert between different units (mg, mcg, IU)?
1 mg equals 1,000 mcg. To convert mg to mcg, multiply by 1,000. To convert mcg to mg, divide by 1,000. International Units (IU) are compound-specific and require a conversion factor provided by the manufacturer. For example, somatropin is approximately 3 IU per 1 mg, but this varies by formulation and must never be assumed for other peptides.
What should I do if my calculated draw volume is less than 5 units on an insulin syringe?
Reconstitute with more bacteriostatic water to reduce the concentration, which increases the draw volume into a more accurately measurable range. For example, if your calculation yields 3 units (0.03 mL), doubling the reconstitution volume halves the concentration and doubles the draw volume to 6 units (0.06 mL), improving measurement accuracy.
How long can I store lyophilised peptides before reconstitution?
Lyophilised peptides stored at -20°C in sealed vials protected from moisture and light remain stable until the expiry date, typically 2–3 years from manufacture. Once a vial is opened or removed from frozen storage, it should be reconstituted promptly and not returned to the freezer, as condensation during thawing introduces moisture that degrades the peptide.
Do I need to adjust dosing for peptides with different purity levels?
For peptides above 98% purity, adjustment is optional and the error from neglecting purity is typically smaller than measurement error. For peptides below 95% purity, adjust the amount of lyophilised material used to account for inactive components: divide the target dose by the purity percentage to determine how much total material to use.
Can I mix different peptides in the same vial?
Mixing peptides is not recommended unless specifically validated for the combination. Different peptides may have incompatible solubility requirements, pH optima, or stability characteristics. Chemical interactions between peptides can cause aggregation or degradation. Prepare and store each peptide separately, then draw and mix immediately before administration if the protocol requires co-administration.
What is the best injection site for subcutaneous peptide administration in rodents?
The dorsal neck region (scruff) is the standard subcutaneous injection site for rodents because it is easily accessible, has loose skin that accommodates injection volume, and is difficult for the animal to reach, reducing the risk of the animal disturbing the injection site. Abdominal subcutaneous injections are an alternative but may show different absorption kinetics.
How do I know if my peptide has degraded?
Visual signs include cloudiness, visible particles, colour change, or unusual odour. However, many forms of degradation are not visually apparent. The most reliable indicator is time: discard reconstituted peptides after 14 days regardless of appearance. For critical applications, analytical testing (HPLC or mass spectrometry) can definitively measure remaining active peptide.
Should I draw air into the vial before withdrawing peptide solution?
Yes, injecting air equal to the volume you plan to withdraw equalises pressure in the vial and makes drawing the solution easier. Without this step, a vacuum forms in the vial as you withdraw solution, making it difficult to pull the plunger and potentially causing inaccurate measurement.
What happens if I accidentally inject air instead of peptide solution?
A small air bubble (under 0.1 mL) injected subcutaneously is generally harmless and will be absorbed without effect. Larger air volumes can cause discomfort and may affect absorption kinetics by creating a gas pocket that separates the peptide from surrounding tissue. Always expel air bubbles before injection by tapping the syringe and pushing the plunger until liquid appears at the needle tip.
Can I reuse syringes for multiple doses from the same vial?
No. Syringes and needles are single-use items. Reusing syringes introduces contamination risk, dulls the needle (causing tissue damage and pain), and may transfer material between vials if you use the same syringe for different peptides. Always use a fresh sterile syringe for each dose.
Accurate peptide dosage calculation for research requires systematic attention to concentration determination, unit conversions, and measurement technique. The core workflow—calculating concentration from peptide amount and dilution volume, converting the target dose to the appropriate units, and determining the draw volume—applies universally across peptides and research models. Weight-based dosing scales for subject size, while fixed-amount dosing maintains consistency across standardised cohorts.
Reconstitution technique directly affects concentration accuracy: inject bacteriostatic water slowly down the vial wall, swirl gently until dissolved, and label immediately with concentration and date. Choose reconstitution volume to place typical draw volumes in the 0.1–0.5 mL range where insulin syringe accuracy is highest. For doses requiring less than 5 units, reconstitute to a lower concentration to increase draw volume into the measurable range.
Storage conditions determine peptide stability and dosing consistency throughout a study. Refrigerate reconstituted peptides at 2–8°C, protect from light, and use within 14 days. For studies exceeding 14 days, prepare fresh vials at two-week intervals rather than attempting degradation corrections. Store lyophilised peptides at -20°C until ready for reconstitution.
Species-specific considerations matter for rodent models: mice and rats require different absolute doses even at the same mcg/kg specification due to metabolic rate differences. Administration route affects bioavailability and dosing frequency: subcutaneous injection provides sustained absorption with 50–90% bioavailability, while intravenous administration delivers 100% bioavailability with immediate peak concentration. Dosing frequency depends on peptide half-life, with compounds under four-hour half-lives requiring multiple daily doses and those exceeding eight hours supporting once-daily protocols.
Verification prevents costly errors: double-check calculations, have a colleague independently verify concentration and draw volume, maintain detailed dosing logs, and periodically validate syringe accuracy. For research requiring maximum precision, consider analytical verification of reconstituted concentration via HPLC.
Sempica provides research-grade peptides manufactured to 99.8% purity with full analytical documentation, supporting accurate dosing calculations and reproducible research outcomes. All compounds are supplied with Certificates of Analysis and detailed reconstitution guidance. For specific peptide protocols and additional technical resources, explore our research compound catalogue and laboratory guides.
Products sold on this website are intended for research purposes only. They are not for human consumption, medical use, or therapeutic application. By purchasing from this website, you confirm that you are a qualified professional and will use these products strictly for laboratory research.
[1] Peptide Dosage – https://www.omnicalculator.com/health/peptide-dosage
[2] Dosing Guidelines – https://deltapeptides.com/dosing-guidelines.html
[3] Peptide Calculator – https://primepeptides.co/peptide-calculator/
[4] Peptides Dosage Calculator – https://dnlabresearch.com/peptides-dosage-calculator/
[6] peptidedosages – https://peptidedosages.com
SEO Meta Title: How to Calculate Peptide Dosage for Research | 2026 Guide
Unsure of How much of Ozempic of
Planning to take your first shot of

Are Storing Ozempic in your Refrigerator? How