Semaglutide vs tirzepatide which is better for weight loss
Semaglutide vs tirzepatide which is better for
Quick Answer
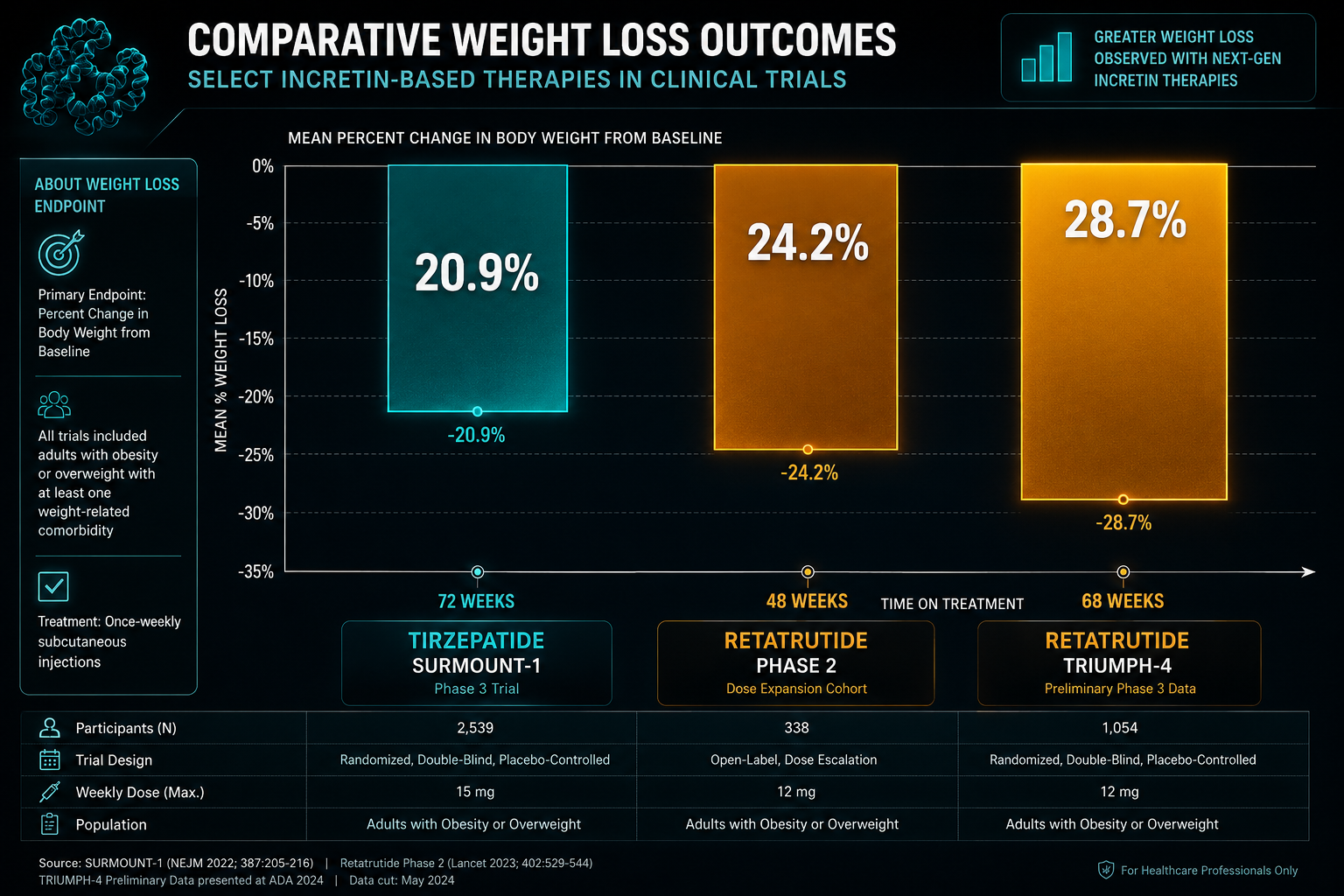
Tirzepatide is a dual GLP-1/GIP receptor agonist with FDA approval and well-documented clinical trial data, including a mean body weight reduction of approximately 20.9% over 72 weeks in the SURMOUNT-1 trial. Retatrutide adds a third mechanism — glucagon receptor activation — and Phase 2 data suggest it may produce greater weight reduction (approximately 24.2% at 48 weeks), though it remains investigational as Phase 3 TRIUMPH trials continue. For researchers comparing tirzepatide vs retatrutide research outcomes, the core distinction is receptor breadth: two pathways versus three, and what that difference means for metabolic and body composition endpoints.
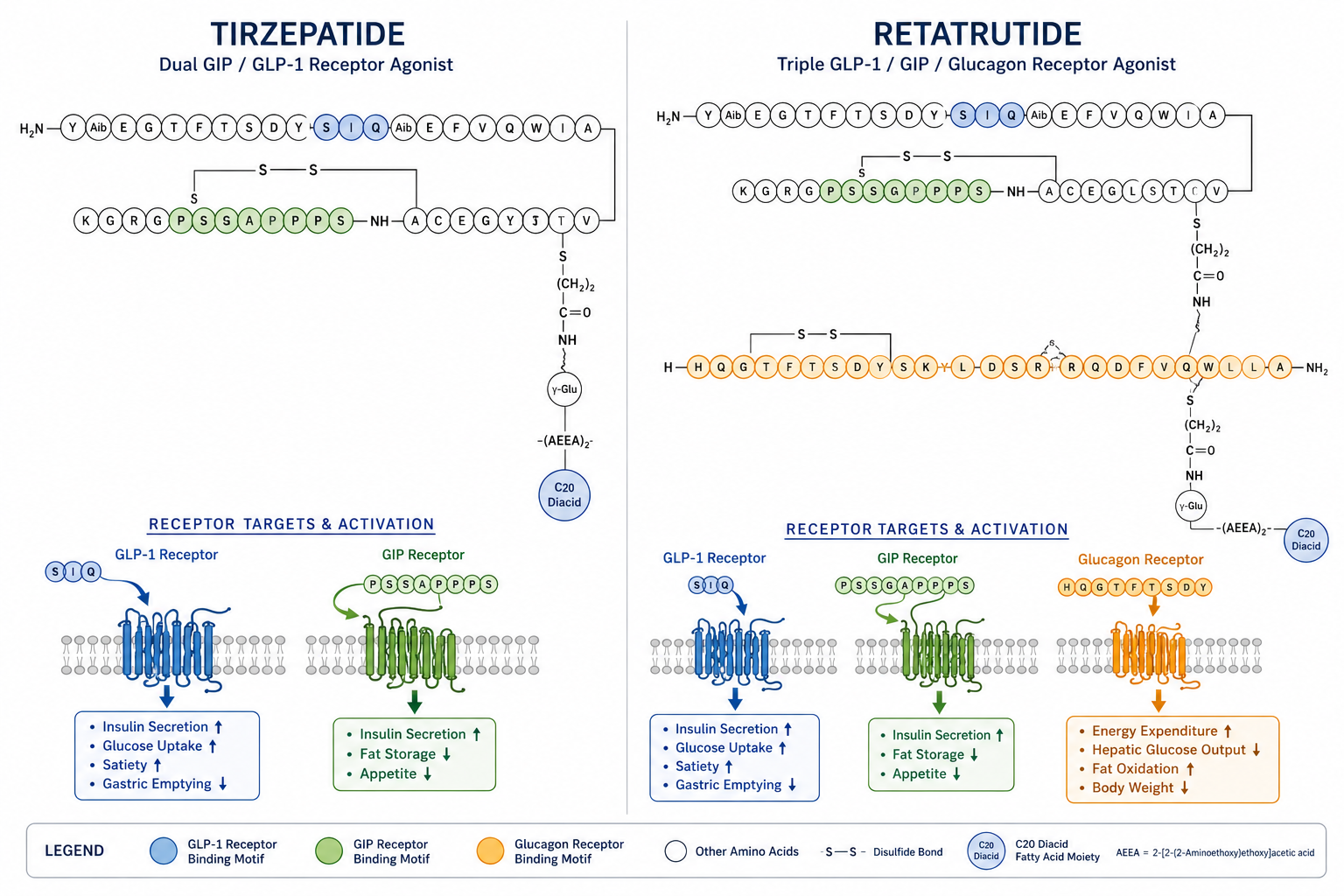
Tirzepatide is a synthetic 39-amino acid peptide that acts as a dual agonist at both the GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide) receptors. Retatrutide is a synthetic peptide that activates those same two receptors plus the glucagon receptor, making it a triple agonist and the most mechanistically broad incretin-based compound currently in advanced research. [1][3]
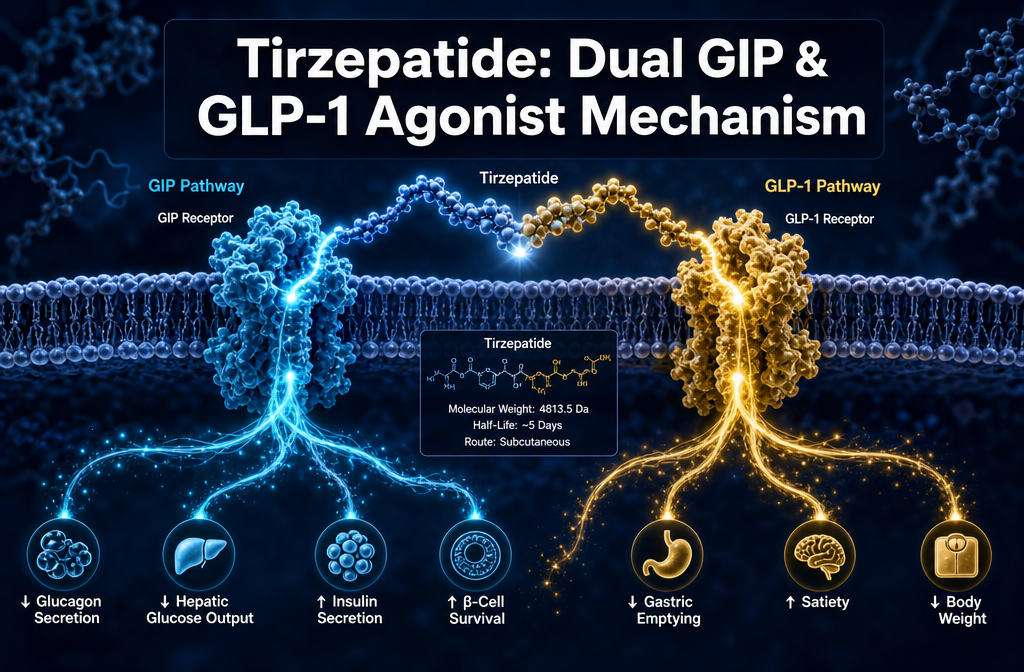
Tirzepatide mechanism: By co-activating GLP-1 and GIP receptors, tirzepatide stimulates insulin secretion in a glucose-dependent manner, suppresses glucagon release, slows gastric emptying, and reduces appetite signalling in the hypothalamus. The addition of GIP agonism appears to produce additive effects on fat metabolism and insulin sensitivity beyond what GLP-1 agonism alone achieves — a key finding that distinguished tirzepatide from earlier GLP-1 monotherapy compounds.
Retatrutide mechanism: The glucagon receptor component is what separates retatrutide from tirzepatide in mechanistic terms. Glucagon receptor activation increases energy expenditure and promotes lipolysis, meaning retatrutide acts on three distinct metabolic levers simultaneously. [1] In preclinical and early clinical research, this triple-pathway activity has been associated with greater reductions in both body weight and hepatic fat compared to dual-agonist approaches.
For researchers exploring multi-pathway metabolic research, Sempica’s dedicated GLP-1/GIP multi-pathway metabolic research peptides resource provides additional mechanistic context for both compound classes.
Based on available data, retatrutide appears to produce greater percentage weight loss than tirzepatide, though a direct head-to-head randomised controlled trial has not yet been published. Both compounds show outcomes that substantially exceed those of earlier GLP-1 monotherapy agents.
Tirzepatide (SURMOUNT-1 trial):
Retatrutide Phase 2 trial:
Retatrutide Phase 3 (TRIUMPH-4, preliminary):
“The addition of glucagon receptor agonism in retatrutide appears to shift the efficacy ceiling meaningfully upward relative to dual-agonist approaches — a finding that has significant implications for body composition research models.”
Comparing these figures requires methodological caution. The trials used different durations, populations, and titration schedules, so the numbers are not directly equivalent. Nonetheless, the pattern across tirzepatide vs retatrutide research outcomes consistently places retatrutide at a higher weight reduction endpoint.
In the SURMOUNT-1 trial, approximately 56% of tirzepatide participants at the 15 mg dose achieved at least 20% body weight reduction over 72 weeks. [1] Retatrutide Phase 2 data showed that the majority of participants at the 12 mg dose exceeded 20% weight loss by week 48, with a mean reduction of 24.2%. [2]
These response rates are substantially higher than those observed with semaglutide (approximately 14.9% mean weight loss in the STEP 1 trial at 2.4 mg weekly), which positions both tirzepatide and retatrutide as higher-efficacy compounds within the incretin class for body composition research endpoints.
Tirzepatide and retatrutide both outperform semaglutide on weight reduction endpoints in available trial data, with the mechanistic explanation lying in receptor breadth.
| Compound | Receptor Targets | Approx. Mean Weight Loss | Regulatory Status (2026) |
|---|---|---|---|
| Semaglutide | GLP-1 | ~14.9% (72 weeks, STEP 1) | FDA-approved |
| Tirzepatide | GLP-1 + GIP | ~20.9% (72 weeks, SURMOUNT-1) | FDA-approved |
| Retatrutide | GLP-1 + GIP + Glucagon | ~24.2% (48 weeks, Phase 2) | Investigational |
Semaglutide remains the most extensively studied compound in this class and carries the most robust long-term cardiovascular outcome data (SUSTAIN-6, SELECT trials). Tirzepatide’s SURPASS-CVOT trial demonstrated noninferiority to dulaglutide on cardiovascular endpoints. [2] Retatrutide’s long-term cardiovascular data are still emerging from Phase 3 investigations.
Researchers interested in semaglutide as a comparator compound can review Sempica’s semaglutide research compound specifications alongside the broader metabolic and energy research compounds catalogue.
Both compounds share a predominantly gastrointestinal side effect profile, consistent with the GLP-1 receptor agonist class. The key clinical difference is that retatrutide introduces an additional adverse event — dysesthesia — not prominently observed with tirzepatide. [2][3]
Common to both compounds:
Retatrutide-specific observations:
Side effects in both compounds are generally dose-dependent and most pronounced during dose escalation phases. Gradual titration protocols in trials were designed specifically to reduce gastrointestinal burden during the initial weeks of administration.
In clinical trials, both compounds are administered via weekly subcutaneous injection with structured dose escalation protocols.
Tirzepatide (SURMOUNT-1 protocol):
Retatrutide (Phase 2 protocol):
Researchers designing preclinical or comparative studies should note that these protocols were developed specifically to manage tolerability. Dose escalation timelines are not interchangeable between compounds, and the pharmacokinetic profiles differ — tirzepatide has a half-life of approximately 5 days, while retatrutide’s half-life is approximately 6 days.
For researchers sourcing retatrutide for laboratory investigation, Sempica offers both retatrutide 20 mg and retatrutide 40 mg research formulations, as well as tirzepatide 30 mg and tirzepatide 60 mg options.
Tirzepatide has the stronger evidence base for type 2 diabetes research, backed by FDA approval (Mounjaro, 2022) and multiple completed Phase 3 SURPASS trials demonstrating significant HbA1c reductions. [2][3] Retatrutide also shows meaningful glycaemic effects in Phase 2 data, but its diabetes-specific trial programme is less mature.
In the SURPASS trial series, tirzepatide consistently reduced HbA1c by 1.8–2.4 percentage points across doses, with a proportion of participants achieving normoglycaemia. The dual GIP/GLP-1 mechanism is particularly relevant here because GIP receptors are expressed on pancreatic beta cells and contribute to glucose-dependent insulin secretion independently of GLP-1.
Retatrutide’s glucagon receptor agonism introduces a theoretical complexity in diabetes models: glucagon typically raises blood glucose, and its receptor activation requires careful interpretation in glycaemic research contexts. Phase 2 data suggest this is offset by the dominant insulin-stimulating effects of the GLP-1 and GIP components, but researchers should account for this mechanistic nuance when designing diabetes-focused protocols.
One of the most striking findings in tirzepatide vs retatrutide research outcomes relates to hepatic fat reduction. Retatrutide has demonstrated up to 82–86% relative reduction in liver fat in a Phase 2 trial involving patients with metabolic-associated steatotic liver disease (MASLD). [2] This positions it as a particularly relevant compound for liver metabolism and MASLD research models.
Tirzepatide has also shown significant liver fat reduction in metabolic studies, consistent with its GLP-1 and GIP mechanisms. However, the magnitude of hepatic fat reduction reported for retatrutide in the MASLD-specific trial exceeds what has been documented for tirzepatide in comparable populations.
The glucagon receptor pathway is likely a contributing factor here: glucagon signalling promotes hepatic fatty acid oxidation and reduces lipogenesis, effects that complement the insulin-sensitising actions of GLP-1 and GIP agonism. For researchers investigating non-alcoholic fatty liver disease models or broader hepatic lipid metabolism, this distinction in tirzepatide vs retatrutide research outcomes is scientifically significant.
Tirzepatide is fully FDA-approved for two indications: type 2 diabetes management (Mounjaro, approved 2022) and chronic weight management in adults with obesity or overweight with at least one weight-related comorbidity (Zepbound, approved 2023). [2] It also holds approvals in the EU and other major markets.
Retatrutide remains investigational as of mid-2026. Phase 3 TRIUMPH trials are ongoing, and regulatory submission is anticipated pending successful trial completion. Approval has been projected for mid-2026 to early 2027, though this timeline is subject to trial outcomes and regulatory review timelines. [3]
This regulatory distinction matters for research design: tirzepatide has an established clinical comparator dataset and approved dosing framework, while retatrutide research remains within the clinical development context. Researchers using retatrutide in preclinical models are working with a compound whose full Phase 3 profile is still being characterised.
Long-term safety data are more extensive for tirzepatide, given its approved status and post-market surveillance. The SURPASS-CVOT trial established cardiovascular noninferiority to dulaglutide, and ongoing post-approval studies continue to build the long-term safety dataset. [2] Known class-related concerns include potential thyroid C-cell effects (observed in rodent models with GLP-1 agonists, not confirmed in humans), pancreatitis risk, and gastrointestinal tolerability.
For retatrutide, long-term safety data are limited to Phase 2 and early Phase 3 observations. The dysesthesia signal at higher doses warrants continued monitoring. The glucagon receptor component introduces additional research questions around bone density (glucagon has known effects on calcium metabolism) and cardiac function, both of which are being evaluated in ongoing trials.
Researchers designing long-duration preclinical studies should account for these open questions when selecting endpoints and monitoring parameters. The absence of long-term human data for retatrutide does not preclude its use in research models but does underscore the importance of rigorous experimental design.
In clinical trial data, both compounds produce measurable weight reduction within the first 4–8 weeks of administration, with the steepest rate of loss typically occurring during the active dose escalation phase.
Tirzepatide timeline (SURMOUNT-1):
Retatrutide timeline (Phase 2):
The faster early trajectory observed with retatrutide in Phase 2 data may reflect the additive energy expenditure effects of glucagon receptor activation, though this hypothesis requires confirmation in controlled comparative studies.
Q: Is retatrutide stronger than tirzepatide?
A: Available Phase 2 data suggest retatrutide produces greater weight reduction (approximately 24.2% at 48 weeks versus tirzepatide’s 20.9% at 72 weeks), but a direct head-to-head trial has not been published. The mechanistic difference — triple versus dual receptor agonism — supports the efficacy advantage, but the comparison is not yet definitive. [1][2]
Q: Has retatrutide been approved by the FDA?
A: No. As of mid-2026, retatrutide remains investigational. Phase 3 TRIUMPH trials are ongoing, and approval is anticipated in mid-2026 to early 2027, pending trial outcomes. [3]
Q: What makes retatrutide different from tirzepatide mechanistically?
A: Retatrutide adds glucagon receptor agonism to the GLP-1 and GIP receptor activation shared with tirzepatide. This third pathway enhances energy expenditure and lipolysis, which is believed to account for its higher observed weight reduction in research. [1]
Q: Can tirzepatide and retatrutide be used together in research?
A: No published data support combination use of these two compounds. Research protocols should treat them as distinct investigational agents for comparative or individual pathway studies.
Q: What is the half-life difference between tirzepatide and retatrutide?
A: Tirzepatide has a half-life of approximately 5 days; retatrutide has a half-life of approximately 6 days. Both support once-weekly administration in research protocols.
Q: Which compound has better liver fat reduction data?
A: Retatrutide has demonstrated up to 82–86% relative reduction in liver fat in a Phase 2 MASLD trial, which exceeds documented tirzepatide data in comparable populations. [2]
Q: Are these compounds available for preclinical research?
A: Yes. Both are available as research compounds for qualified laboratory professionals. Sempica supplies both at 99.8% purity with independent Certificates of Analysis. All products are strictly for research use and not for human consumption.
Q: What side effect distinguishes retatrutide from tirzepatide?
A: Dysesthesia — abnormal skin sensations including tingling or burning — has been reported in up to 20.9% of retatrutide participants at the 12 mg dose. This has not been prominently reported with tirzepatide. [2]
Q: How does tirzepatide compare to semaglutide in weight loss research?
A: Tirzepatide produces approximately 20.9% mean weight loss versus semaglutide’s approximately 14.9% in respective trials, attributable to the additional GIP receptor pathway. These figures come from different trials and should not be treated as a direct comparison.
Q: Where can researchers source these compounds for laboratory use?
A: Sempica Healthcare supplies both tirzepatide and retatrutide as high-purity research compounds verified to 99.8% purity. Researchers can review the full catalogue and compound specifications at sempicahealthcare.ch.
The comparison of tirzepatide vs retatrutide research outcomes points clearly in one direction: each additional receptor pathway appears to translate into measurable gains in metabolic efficacy endpoints. Tirzepatide’s dual GLP-1/GIP mechanism set a new benchmark when its SURMOUNT-1 data were published, and retatrutide’s triple-agonist profile has since extended that benchmark further in Phase 2 and early Phase 3 data.
For research professionals, the practical implications are as follows:
The field is moving rapidly. Full Phase 3 TRIUMPH data for retatrutide, when published, will either confirm or refine the efficacy picture suggested by Phase 2 results. Researchers designing protocols now should build in flexibility to incorporate updated data as it becomes available.
Sempica supplies both compounds as lyophilised research powders at 99.8% purity, independently verified by Certificate of Analysis, and available to qualified research professionals globally. For broader context on the incretin research landscape, the GLP-1/GIP multi-pathway metabolic research peptides resource and the metabolic and energy research compounds catalogue provide additional compound-level detail to support protocol development.
Research Use Disclaimer: All products referenced in this article are intended for research purposes only. They are not for human consumption, medical use, or therapeutic application. By purchasing from sempicahealthcare.ch, you confirm that you are a qualified professional and will use these products strictly for laboratory research.
[1] Retatrutide Vs Tirzepatide Research – https://www.retalabs.is/research/retatrutide-vs-tirzepatide-research?utm_source=openai
[2] Tirzepatide Vs Retatrutide – https://peptidepedia.org/guides/tirzepatide-vs-retatrutide?utm_source=openai
[3] How Retatrutide Compare Tirzepatide 3580916 – https://www.drugs.com/medical-answers/how-retatrutide-compare-tirzepatide-3580916/?utm_source=openai
Semaglutide vs tirzepatide which is better for

Confused on Retatrutide vs Tirzepatide for weight
What is Tirzepatide dual GIP GLP-1 agonist