
How to calculate peptide dosage for peptide
Unsure of How much of Ozempic of
Quick Answer
Semaglutide is a synthetic 31-amino acid peptide that functions as a GLP-1 (glucagon-like peptide-1) receptor agonist, designed for metabolic research applications including glucose homeostasis, insulin signalling, and appetite regulation studies. The compound works by selectively binding to and activating GLP-1 receptors in pancreatic beta cells, the gastrointestinal tract, and the central nervous system, producing effects on insulin secretion, glucagon suppression, gastric emptying, and hypothalamic appetite signalling. With an extended half-life of approximately seven days due to structural modifications including acylation with a C18 fatty diacid chain, semaglutide enables once-weekly administration protocols in research settings.
Semaglutide is a synthetic peptide analogue of human glucagon-like peptide-1 (GLP-1), consisting of 31 amino acids with specific structural modifications that distinguish it from the endogenous hormone. The compound belongs to the incretin mimetic class and functions as a selective GLP-1 receptor agonist in metabolic research applications.
The peptide shares 94% sequence homology with native human GLP-1 but incorporates two critical modifications: an amino acid substitution at position 8 (alanine replaced with alpha-aminoisobutyric acid) and acylation at position 26 via a spacer and C18 fatty diacid chain. These structural alterations serve specific functional purposes in research protocols.
Key structural features:
The acylation modification enables reversible binding to serum albumin, which significantly extends the compound’s plasma half-life compared to native GLP-1 (which has a half-life of approximately two minutes). This albumin binding also reduces renal clearance and protects the peptide from rapid enzymatic breakdown, making semaglutide suitable for once-weekly administration protocols in research models.
The compound is synthesized using solid-phase peptide synthesis techniques and supplied as a sterile, white to off-white lyophilised powder at 99.8% purity. Each batch undergoes independent third-party testing to verify identity, purity, and potency through high-performance liquid chromatography (HPLC) and mass spectrometry analysis.
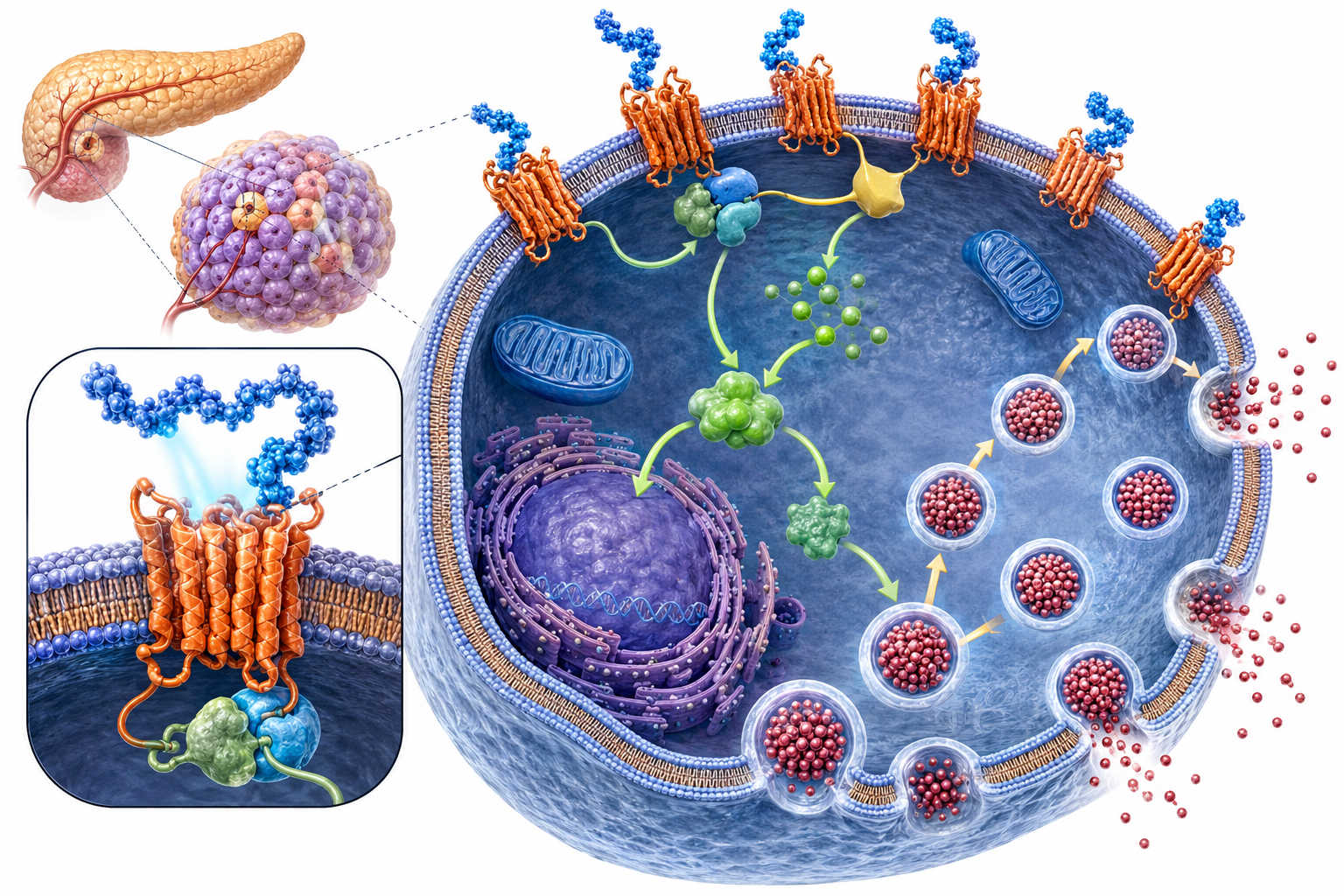
Semaglutide exerts its effects by selectively binding to and activating the GLP-1 receptor, a G-protein coupled receptor (GPCR) expressed in multiple tissue types including pancreatic islet cells, gastrointestinal epithelium, cardiovascular tissue, and specific regions of the central nervous system. Upon receptor activation, semaglutide initiates a cascade of intracellular signalling events that modulate glucose homeostasis, energy metabolism, and appetite regulation.
Primary mechanisms in metabolic research:
Pancreatic beta cell activation: Semaglutide binding to GLP-1 receptors on pancreatic beta cells triggers adenylyl cyclase activation and increased cyclic AMP (cAMP) production. This second messenger cascade enhances glucose-dependent insulin secretion, meaning insulin release occurs only when blood glucose concentrations are elevated. This glucose-dependent mechanism is a key feature in research models examining glycemic control without hypoglycemic risk.
Glucagon suppression: The compound simultaneously inhibits glucagon secretion from pancreatic alpha cells through GLP-1 receptor-mediated pathways. Reduced glucagon output decreases hepatic glucose production, contributing to improved glucose homeostasis in metabolic research models.
Gastric emptying modulation: GLP-1 receptor activation in the gastrointestinal tract slows gastric emptying through effects on gastric smooth muscle and pyloric sphincter tone. This delayed nutrient absorption affects postprandial glucose excursions and contributes to satiety signalling in appetite regulation studies.
Central nervous system effects: Semaglutide crosses the blood-brain barrier and activates GLP-1 receptors in hypothalamic regions involved in appetite control, particularly the arcuate nucleus and paraventricular nucleus. This central activation reduces food intake through modulation of pro-opiomelanocortin (POMC) and neuropeptide Y (NPY) neuronal pathways.
Cardiovascular tissue effects: GLP-1 receptors are expressed in cardiac myocytes, vascular endothelium, and smooth muscle. Research indicates semaglutide may influence cardiovascular function through effects on endothelial function, inflammation markers, and cardiac metabolism, making it relevant for cardiovascular outcome studies.
The compound’s extended half-life of approximately seven days results from three pharmacokinetic features: albumin binding (reducing free drug clearance), DPP-4 resistance (preventing enzymatic degradation), and reduced renal filtration (due to the large albumin-bound complex). These properties enable sustained receptor activation with once-weekly administration in research protocols.
For researchers interested in metabolic pathway research compounds, understanding semaglutide’s selective GLP-1 receptor agonism provides context for comparing it with dual and triple agonist compounds.
Semaglutide serves multiple research applications across metabolic science, cardiovascular studies, and neurological investigations. The compound’s primary use in laboratory settings focuses on understanding GLP-1 receptor-mediated pathways and their effects on whole-body metabolism, energy homeostasis, and tissue-specific responses.
Core research applications:
Metabolic pathway studies: Researchers use semaglutide to investigate glucose homeostasis mechanisms, insulin sensitivity modulation, and hepatic glucose production. The compound enables examination of GLP-1 receptor signalling cascades and their downstream effects on metabolic gene expression, enzyme activity, and substrate utilization patterns.
Insulin resistance models: Semaglutide provides a tool for studying insulin resistance reversal mechanisms and beta cell function preservation in metabolic disease models. Research protocols examine how GLP-1 receptor activation affects insulin receptor signalling, glucose transporter expression, and intracellular glucose metabolism.
Appetite regulation research: The compound’s effects on hypothalamic appetite circuits make it valuable for investigating central nervous system control of food intake, energy expenditure, and body weight regulation. Studies examine neuronal activation patterns, neuropeptide expression, and reward pathway modulation.
Cardiovascular outcome investigations: Research applications include examination of GLP-1 receptor effects on endothelial function, atherosclerosis progression, cardiac remodelling, and inflammatory marker expression. Semaglutide enables study of potential cardioprotective mechanisms independent of glucose-lowering effects.
Body composition research: Laboratory investigations use semaglutide to study fat mass reduction, lean mass preservation, and adipose tissue metabolism. Research examines lipolysis activation, adipokine secretion, and brown adipose tissue thermogenesis.
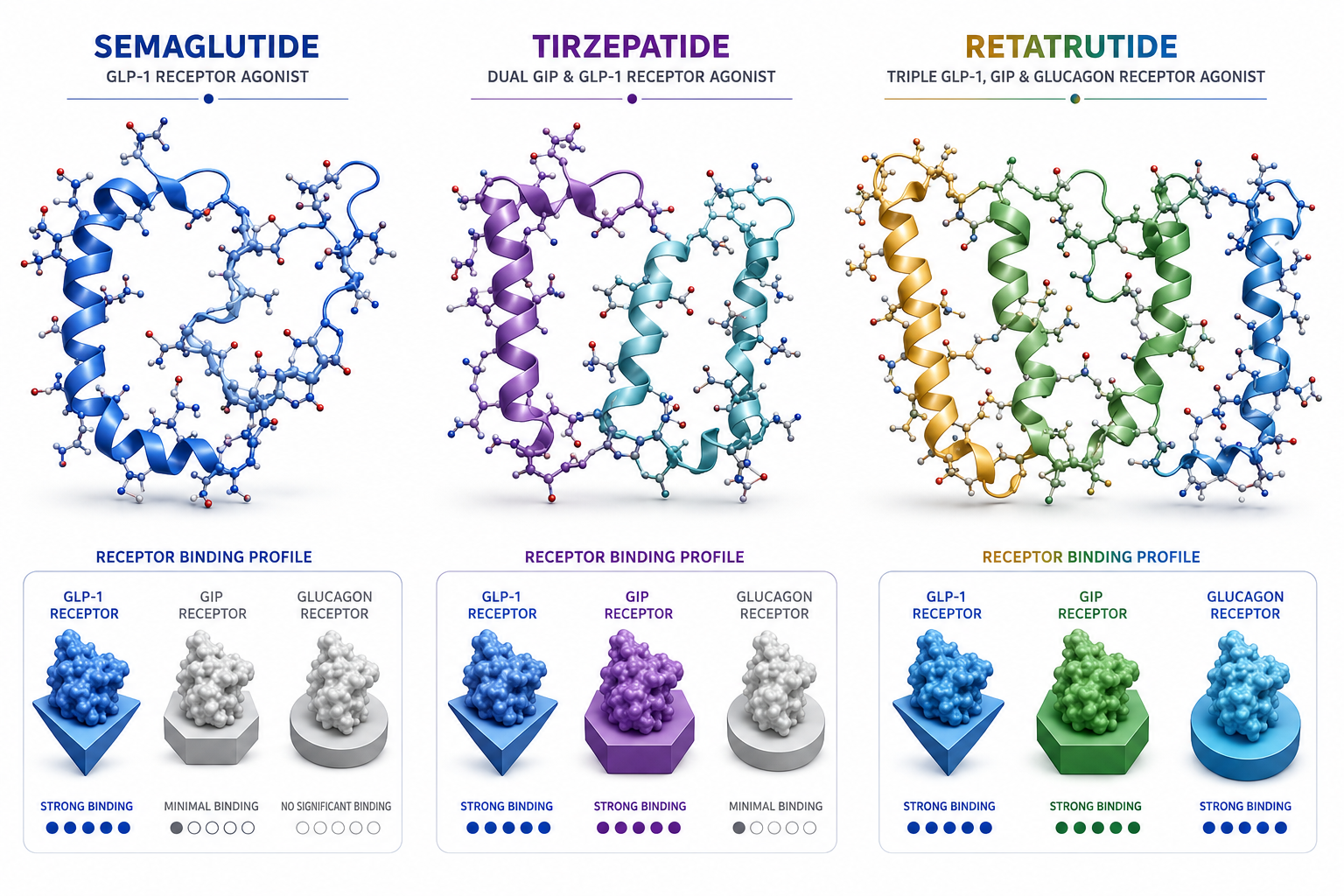
Comparative pharmacology studies: Semaglutide serves as a reference compound for comparing selective GLP-1 agonism against dual GIP/GLP-1 agonists (like tirzepatide) and triple agonists (like retatrutide), enabling researchers to dissect individual receptor pathway contributions to metabolic outcomes.
Cognitive function research: Emerging research applications examine GLP-1 receptor activation effects on neuroinflammation, synaptic plasticity, and neurodegenerative disease models, particularly in studies exploring metabolic-cognitive connections.
All research applications must be conducted by qualified professionals in controlled laboratory settings. Sempica supplies semaglutide strictly for research purposes, and all products carry the mandatory research-use-only designation. Researchers should consult the comprehensive laboratory guide on peptide handling for proper reconstitution and storage protocols.
Semaglutide produces significant body weight reduction in research models through multiple complementary mechanisms that affect both energy intake and energy expenditure. Laboratory studies demonstrate that GLP-1 receptor activation creates a negative energy balance by reducing caloric consumption while potentially increasing metabolic rate.
The primary mechanism involves central nervous system appetite suppression. Semaglutide activates GLP-1 receptors in the arcuate nucleus of the hypothalamus, increasing pro-opiomelanocortin (POMC) neuronal activity while decreasing neuropeptide Y (NPY) and agouti-related peptide (AgRP) signalling. This neuronal shift reduces hunger perception and increases satiety signals, leading to decreased food intake in research subjects.
Weight loss mechanisms in research:
Research protocols examining body composition changes typically observe dose-dependent weight reduction, with higher doses producing greater magnitude effects. Studies indicate that weight loss continues for approximately 60-70 weeks before reaching a plateau, after which weight stabilizes at the new lower set point.
The compound’s effects on adipose tissue extend beyond simple caloric deficit. Research shows GLP-1 receptor activation influences adipocyte metabolism, promoting lipolysis (fat breakdown) and potentially reducing lipogenesis (fat synthesis). Some studies indicate effects on brown adipose tissue activation, which increases thermogenic energy expenditure.
Importantly, research demonstrates that weight loss achieved through semaglutide administration reverses when the compound is discontinued, with subjects typically regaining 50-70% of lost weight within one year of cessation. This rebound effect is a critical consideration in research design and indicates that the compound’s effects are pharmacological rather than producing permanent metabolic reprogramming.
For researchers comparing weight loss mechanisms across different compound classes, examining semaglutide alongside dual-pathway metabolic research compounds provides insight into how additional receptor agonism (GIP, glucagon) affects body composition outcomes.
Semaglutide and Ozempic are not different compounds—Ozempic is a brand name for semaglutide formulated and marketed for type 2 diabetes management. The confusion arises because the same active pharmaceutical ingredient (semaglutide) is sold under multiple brand names for different approved indications, but the molecular structure remains identical.
Brand name distinctions:
The active compound in all three products is semaglutide with identical molecular structure and mechanism of action. The distinction lies in formulation (injectable vs. oral), dosing protocols, and regulatory approval indications. Injectable formulations (Ozempic, Wegovy) use the same subcutaneous delivery method but differ in maximum approved doses and prescribing indications.
For research purposes, these brand distinctions are irrelevant. Laboratory researchers use pure semaglutide compound without brand-specific formulation additives. Sempica supplies research-grade semaglutide as lyophilised powder at 99.8% purity, enabling researchers to design custom protocols without the constraints of commercial formulations.
Key research considerations:
The recent development of oral semaglutide formulations (Rybelsus, and newer high-dose oral formulations) represents a significant advancement in delivery technology. These formulations incorporate absorption enhancers (specifically, sodium N-(8-[2-hydroxybenzoyl] amino) caprylate or SNAC) that facilitate peptide absorption across the gastric epithelium, overcoming the typical degradation of peptides in the gastrointestinal tract.
For researchers examining formulation effects on bioavailability and pharmacokinetics, comparing subcutaneous versus oral delivery routes provides valuable data on absorption kinetics, first-pass metabolism, and tissue distribution patterns.
Semaglutide demonstrates time-dependent effects that vary by measured outcome, with different physiological responses occurring across distinct timeframes. Understanding these temporal patterns is essential for research protocol design and endpoint selection.
Immediate effects (hours to days): GLP-1 receptor activation occurs within hours of first administration, producing measurable effects on insulin secretion and glucagon suppression in response to glucose challenge. Gastric emptying delay is detectable within 24-48 hours of initial dosing.
Early metabolic effects (1-2 weeks): Fasting glucose levels begin declining within the first week of administration in metabolic research models. Postprandial glucose excursions show improvement within 7-10 days. These early glycemic effects occur before significant body weight changes.
Appetite suppression onset (1-4 weeks): Central nervous system effects on appetite typically manifest within 1-2 weeks, with maximal appetite suppression occurring after 3-4 weeks at stable dosing. Food intake reduction follows a gradual pattern rather than immediate onset.
Body weight reduction (4-60 weeks): Measurable weight loss typically begins after 2-4 weeks, with linear weight reduction continuing for approximately 60-70 weeks before reaching plateau. The rate of weight loss averages 0.5-1.0% of body weight per week during the active reduction phase.
Steady-state pharmacokinetics (4-5 weeks): Due to semaglutide’s seven-day half-life, steady-state plasma concentrations are achieved after approximately 4-5 weeks of weekly dosing. This means full pharmacological effects are not realized until the compound accumulates to equilibrium levels.
Cardiovascular markers (12-24 weeks): Research examining cardiovascular endpoints (inflammatory markers, endothelial function, blood pressure) typically requires 12-24 weeks to detect significant changes, as these represent secondary effects downstream of metabolic improvements.
Dose escalation considerations: Most research protocols employ gradual dose escalation over 8-16 weeks to minimize gastrointestinal adaptation responses. This titration schedule delays achievement of target dose effects but improves protocol tolerability in research subjects.
Common research timeline:
Research protocols examining acute versus chronic effects should account for these temporal patterns when selecting measurement timepoints. Single-dose studies capture immediate receptor activation and insulin secretion effects, while chronic studies spanning 24-52 weeks are necessary to evaluate body composition, cardiovascular outcomes, and long-term metabolic adaptations.
For researchers designing protocols, consulting the laboratory guide on peptide research protocols provides additional guidance on administration schedules and measurement timing.
Semaglutide administration in research models produces a characteristic profile of physiological responses, some of which may be considered adverse effects depending on research objectives. Understanding these responses is essential for protocol design, subject monitoring, and data interpretation.
Gastrointestinal responses (most common):
Gastrointestinal effects represent the most frequent responses to semaglutide administration, occurring in 30-60% of research subjects depending on dose and titration schedule. These effects result directly from GLP-1 receptor activation in the gastrointestinal tract and central nervous system.
Research protocols can minimize gastrointestinal responses through gradual dose escalation (typically 4-8 week titration schedules) and administration timing relative to feeding schedules.
Metabolic responses:
Pancreatic considerations:
Research has examined potential effects on pancreatic tissue, including pancreatitis occurrence and pancreatic enzyme elevation. While rare in research models, protocols should include pancreatic enzyme monitoring (lipase, amylase) when examining long-term administration effects.
Gallbladder effects:
Some research indicates increased gallstone formation risk with GLP-1 receptor agonists, likely related to rapid weight loss and altered bile composition. Long-term studies may include gallbladder monitoring.
Cardiovascular responses:
Injection site reactions:
Subcutaneous administration may produce local responses including erythema, induration, or mild discomfort at injection sites. Rotating injection sites minimizes these effects.
Thyroid considerations:
Preclinical rodent studies identified thyroid C-cell tumors at high doses, though relevance to other species remains debated. Research protocols examining long-term administration may include thyroid monitoring depending on species and research objectives.
Renal function:
Gastrointestinal effects leading to dehydration may affect renal function markers. Protocols should ensure adequate hydration and monitor renal parameters in long-term studies.
Dose-response relationship:
Most responses demonstrate dose-dependent patterns, with higher doses producing greater frequency and severity. Gradual dose escalation significantly reduces response incidence compared to immediate high-dose administration.
Adaptation patterns:
Many responses, particularly gastrointestinal effects, diminish over time as subjects adapt to continued exposure. This adaptation typically occurs over 4-8 weeks at stable dosing.
Research protocols should include appropriate monitoring parameters based on study duration, dose ranges, and specific research objectives. Comparing response profiles across different GLP-1 receptor agonists and multi-pathway agonists provides insight into receptor-specific versus class-wide effects.
Semaglutide and tirzepatide represent different approaches to incretin-based metabolic research, with distinct receptor selectivity profiles that produce overlapping but non-identical effects. Understanding these differences is essential for selecting appropriate compounds for specific research questions.
Receptor selectivity:
This fundamental difference in receptor targeting produces distinct pharmacological profiles despite both compounds affecting glucose homeostasis and body weight regulation.
Mechanism comparison:
Semaglutide activates only GLP-1 receptors, producing effects through the single-pathway mechanisms described earlier: glucose-dependent insulin secretion, glucagon suppression, gastric emptying delay, and central appetite suppression.
Tirzepatide activates both GIP and GLP-1 receptors simultaneously. GIP receptor activation adds complementary effects including enhanced insulin secretion (additive with GLP-1), altered fat metabolism in adipose tissue, and potentially different central nervous system effects on appetite and energy expenditure. The dual agonism produces greater magnitude effects on several metabolic parameters compared to GLP-1 agonism alone.
Comparative research outcomes:
Body weight reduction: Research comparing the two compounds consistently shows tirzepatide produces greater weight loss magnitude (approximately 15-22% body weight reduction) compared to semaglutide (approximately 10-15% reduction) at maximum doses. This difference likely reflects additive effects of GIP receptor activation on metabolism and appetite.
Glycemic control: Both compounds produce robust glucose-lowering effects, with tirzepatide showing slightly greater HbA1c reduction in head-to-head studies. The difference is modest (approximately 0.3-0.5% HbA1c) but statistically significant.
Gastrointestinal tolerability: Both compounds produce similar gastrointestinal response profiles, with nausea and vomiting being most common. Some research suggests tirzepatide may have slightly lower nausea incidence at equivalent efficacy doses, though this remains debated.
Cardiovascular effects: Both compounds demonstrate cardiovascular benefits in research models, though the specific mechanisms may differ due to GIP receptor effects on lipid metabolism and vascular function.
Research applications:
Choose semaglutide when research objectives include:
Choose tirzepatide when research objectives include:
For researchers interested in extending beyond dual agonism, retatrutide represents a triple GLP-1/GIP/glucagon receptor agonist that adds glucagon receptor activation to further enhance energy expenditure and lipolysis.
Structural differences:
Both compounds are synthetic peptides with albumin-binding modifications for extended half-life, but differ in amino acid sequence and acylation chemistry. Tirzepatide is a 39-amino acid peptide (longer than semaglutide’s 31 amino acids) with a C20 fatty diacid moiety, compared to semaglutide’s C18 chain.
Pharmacokinetic comparison:
Both compounds demonstrate approximately five-day half-lives, enabling once-weekly administration protocols. Steady-state pharmacokinetics are achieved after 4-5 weeks for both compounds. Bioavailability and tissue distribution patterns differ slightly due to structural variations.
Understanding these distinctions enables researchers to select the appropriate compound for specific mechanistic questions and to design comparative studies that dissect individual receptor pathway contributions to metabolic outcomes.
While semaglutide is a research compound rather than a therapeutic agent, certain research model characteristics may contraindicate its use or require modified protocols. Understanding these limitations ensures appropriate research design and subject selection.
Absolute research contraindications:
Personal or family history of medullary thyroid carcinoma: Preclinical rodent studies identified thyroid C-cell tumors (medullary thyroid carcinoma) at high semaglutide doses. While relevance to non-rodent species remains uncertain, research protocols should exclude subjects with relevant thyroid pathology when examining long-term administration effects.
Multiple endocrine neoplasia syndrome type 2 (MEN 2): Related to thyroid concerns, subjects with MEN 2 or family history should be excluded from long-term semaglutide research protocols.
Previous severe hypersensitivity reactions: Subjects demonstrating anaphylaxis or severe allergic responses to semaglutide or structurally similar peptides should be excluded from subsequent protocols.
Relative contraindications and protocol modifications:
Pancreatitis history: Subjects with previous pancreatitis episodes may be inappropriate for semaglutide research, as GLP-1 receptor agonists have been associated with pancreatitis in some studies. If included, protocols should incorporate pancreatic enzyme monitoring.
Severe gastrointestinal disease: Subjects with gastroparesis, inflammatory bowel disease, or other significant gastrointestinal pathology may experience exacerbated symptoms due to semaglutide’s effects on gastric emptying and motility. Research objectives should justify inclusion of such subjects.
Renal impairment: While semaglutide does not require dose adjustment for renal function in most cases, severe renal impairment may affect pharmacokinetics and increase risk of dehydration-related complications. Protocols should include appropriate monitoring.
Hepatic impairment: Limited data exists on semaglutide pharmacokinetics in severe hepatic impairment. Research protocols examining subjects with liver disease should include appropriate safety monitoring.
Pregnancy and lactation: Semaglutide research should exclude pregnant or lactating subjects unless pregnancy/lactation effects are specific research objectives, given limited safety data and potential developmental effects.
Pediatric subjects: Research in pediatric populations requires specialized protocols and ethical considerations, as most semaglutide research has focused on adult subjects.
Diabetic ketoacidosis risk: Subjects with type 1 diabetes or at risk for ketoacidosis require careful protocol design, as semaglutide is not a replacement for insulin and does not prevent ketoacidosis.
Drug interaction considerations:
Semaglutide’s effects on gastric emptying alter absorption kinetics of co-administered compounds. Research protocols examining drug combinations should account for these pharmacokinetic interactions, particularly for compounds with narrow therapeutic windows or time-dependent absorption requirements.
Specific research model considerations:
Rodent models: Thyroid C-cell effects observed in rodent studies may not translate to other species. Researchers should consider species-specific responses when designing protocols and interpreting results.
Cardiovascular research models: Semaglutide’s effects on heart rate and cardiovascular function should be considered when designing protocols examining cardiac physiology or cardiovascular disease models.
Metabolic disease models: Subjects with severe metabolic decompensation may require stabilization before semaglutide administration to isolate compound effects from disease progression.
Protocol design recommendations:
These considerations ensure research protocols are designed with appropriate subject selection criteria and safety monitoring parameters. For researchers designing comprehensive metabolic research protocols, consulting resources on metabolic research compound selection provides additional context for compound choice and protocol design.
Semaglutide administration in research settings requires precise technique to ensure consistent dosing, minimize injection site reactions, and maintain compound stability. Proper subcutaneous injection protocols are essential for reproducible research outcomes.
Reconstitution protocol:
Semaglutide is supplied as lyophilised powder requiring reconstitution before administration. The standard protocol follows these steps:
Subcutaneous injection technique:
Site selection: Semaglutide is administered subcutaneously in areas with adequate subcutaneous fat tissue. Common injection sites include:
Rotate injection sites with each administration to minimize local tissue reactions and prevent lipohypertrophy.
Injection procedure:
Dosing schedule considerations:
Research protocols typically employ once-weekly administration due to semaglutide’s seven-day half-life. Maintain consistent administration timing (same day of week, similar time of day) to minimize pharmacokinetic variability. Administration may occur without regard to feeding schedule, though some protocols standardize timing relative to meals for consistency.
Dose escalation protocols:
Most research protocols employ gradual dose escalation over 4-8 weeks to minimize gastrointestinal responses. A typical escalation schedule might progress: 0.25mg weekly × 4 weeks → 0.5mg weekly × 4 weeks → 1.0mg weekly × 4 weeks → target dose. Adjust escalation speed based on research objectives and subject tolerance.
Quality control measures:
Common technical errors to avoid:
For comprehensive guidance on peptide handling, reconstitution, and storage, researchers should consult the complete laboratory guide to peptide preparation.
Research protocols involving semaglutide frequently encounter preventable errors that compromise data quality, subject welfare, or protocol completion. Understanding these common mistakes enables researchers to design more robust protocols and anticipate potential complications.
Inadequate dose escalation:
The most frequent protocol design error is insufficient dose escalation time. Researchers eager to reach target doses quickly may implement aggressive titration schedules (e.g., weekly dose increases) that produce excessive gastrointestinal responses and protocol discontinuation. Optimal escalation typically requires 4-8 weeks, with some protocols extending to 12-16 weeks for maximum doses. The temporary delay in reaching target dose is offset by improved protocol completion rates and reduced confounding from adverse responses.
Ignoring individual response variability:
Semaglutide produces substantial inter-individual response variability in both efficacy outcomes and adverse effects. Protocol designs that mandate fixed escalation schedules without flexibility for individual tolerance may force premature discontinuation in responsive subjects. Incorporating response-based titration criteria (e.g., “increase dose if gastrointestinal effects are mild or absent”) improves protocol completion while maintaining scientific rigor.
Inadequate baseline characterization:
Failing to establish comprehensive baseline measurements limits ability to detect compound effects and identify confounding variables. Essential baseline parameters include body weight/composition, fasting glucose and insulin, lipid panels, blood pressure, heart rate, gastrointestinal symptom scores, and appetite ratings. Inadequate baseline data prevents proper effect attribution and limits publication potential.
Insufficient monitoring frequency:
Early protocol phases require more frequent monitoring than later maintenance phases. Common errors include:
Improper storage and handling:
Peptide stability is highly sensitive to storage conditions. Frequent mistakes include:
Inadequate hydration protocols:
Semaglutide’s gastrointestinal effects (particularly nausea and vomiting) may reduce fluid intake, leading to dehydration that confounds metabolic measurements and affects renal function markers. Research protocols should include hydration monitoring and standardized fluid intake recommendations.
Failing to account for pharmacokinetic timeline:
Researchers sometimes measure outcomes before steady-state is achieved (requires 4-5 weeks of weekly dosing) or before sufficient time has elapsed for specific effects to manifest. Understanding the temporal patterns described earlier prevents premature outcome assessment and false-negative results.
Inadequate control group design:
Semaglutide research requires careful control group consideration. Common errors include:
Overlooking drug-drug interactions:
Semaglutide’s effects on gastric emptying alter absorption of co-administered compounds. Research examining combination protocols must account for these pharmacokinetic interactions through:
Insufficient statistical power:
Semaglutide produces large effect sizes for some outcomes (body weight, HbA1c) but more modest effects for others (cardiovascular markers, cognitive measures). Researchers sometimes design protocols with adequate power for primary outcomes but insufficient power for secondary endpoints, limiting scientific value.
Neglecting long-term effects:
Short-duration protocols (less than 12 weeks) may miss important temporal patterns including:
Inadequate documentation:
Comprehensive documentation is essential for reproducibility and publication. Common documentation failures include:
Failure to plan for discontinuation effects:
Research protocols should include post-treatment follow-up to characterize rebound effects, weight regain patterns, and metabolic parameter changes after compound cessation. These data are scientifically valuable and essential for complete understanding of compound effects.
Avoiding these common errors requires careful protocol design, adequate pilot studies to identify potential issues, and consultation with experienced researchers. For laboratories new to peptide research, reviewing comprehensive guides on research compound handling and protocol design provides essential foundational knowledge.
Semaglutide discontinuation produces characteristic rebound effects that are important for understanding the compound’s mechanism of action and for designing complete research protocols. These post-treatment effects provide insight into whether semaglutide produces lasting metabolic changes or purely pharmacological effects that reverse upon cessation.
Weight regain patterns:
Research consistently demonstrates that body weight reduction achieved during semaglutide administration reverses substantially after discontinuation. Typical patterns include:
Immediate post-cessation (weeks 1-4): Weight regain begins within 2-4 weeks of final dose as compound plasma levels decline. Initial regain rate is typically 0.3-0.5% body weight per week, slower than the loss rate during active treatment.
Intermediate phase (weeks 4-26): Weight regain accelerates during this period, with subjects typically regaining 50-70% of lost weight within 6 months of discontinuation. The regain rate gradually slows as subjects approach their pre-treatment baseline weight.
Long-term patterns (26+ weeks): Most subjects return to within 5-10% of their pre-treatment weight by 12 months post-discontinuation. Some subjects stabilize at a weight slightly below baseline, while others exceed their original starting weight, though this latter pattern is less common.
Metabolic parameter changes:
Glucose homeostasis: Fasting glucose and HbA1c levels begin rising within 2-4 weeks of discontinuation, typically returning to baseline values within 8-12 weeks. The timeline depends on the degree of weight regain and whether underlying metabolic improvements occurred during treatment.
Insulin sensitivity: Improvements in insulin sensitivity reverse in parallel with weight regain. Research indicates that insulin sensitivity returns to approximately baseline levels once body weight returns to pre-treatment values, suggesting weight loss rather than direct compound effects drove the improvement.
Lipid parameters: Changes in triglycerides, HDL, and LDL cholesterol reverse following discontinuation, with timeline correlating to weight regain patterns. Most lipid parameters return to baseline within 12-24 weeks.
Blood pressure and heart rate: Blood pressure reductions achieved during treatment reverse within 4-8 weeks of discontinuation. Heart rate increases observed during treatment normalize within 2-4 weeks as compound levels decline.
Appetite and food intake:
Central appetite suppression reverses rapidly after discontinuation. Research indicates:
Weeks 1-2: Appetite begins increasing as GLP-1 receptor activation declines. Subjects report increased hunger and reduced satiety compared to on-treatment levels.
Weeks 2-4: Appetite typically exceeds pre-treatment baseline levels, possibly representing a compensatory response to the period of reduced intake. This rebound hunger contributes to rapid weight regain.
Weeks 4-12: Appetite gradually normalizes to pre-treatment levels as metabolic set-point regulation re-establishes baseline patterns.
Gastrointestinal function:
Gastric emptying returns to normal rates within 1-2 weeks of discontinuation as GLP-1 receptor activation ceases. Subjects who experienced constipation during treatment may experience temporary increased bowel frequency as gastrointestinal motility normalizes.
Cardiovascular markers:
Inflammatory markers (CRP, IL-6) and endothelial function measures that improved during treatment typically reverse within 8-16 weeks of discontinuation, correlating with weight regain and metabolic parameter changes.
Mechanisms of rebound effects:
The substantial rebound effects following semaglutide discontinuation indicate that the compound produces pharmacological rather than lasting physiological changes. Several mechanisms contribute:
Metabolic set-point defense: The body’s weight regulation systems actively defend against sustained weight loss through increased hunger, reduced energy expenditure, and metabolic adaptations. When pharmacological appetite suppression is removed, these compensatory mechanisms drive weight regain.
Lack of metabolic reprogramming: Unlike interventions that may produce lasting changes in metabolic regulation (e.g., bariatric surgery), semaglutide does not appear to permanently alter metabolic set-points or regulatory pathways. Effects persist only as long as GLP-1 receptor activation continues.
Adipose tissue memory: Research suggests adipose tissue retains “memory” of previous higher weight states through epigenetic and cellular mechanisms, facilitating rapid weight regain when caloric restriction or appetite suppression ends.
Research protocol implications:
Understanding discontinuation effects is essential for complete research design:
Include post-treatment follow-up: Protocols should incorporate follow-up measurements for at least 12-26 weeks after final dose to characterize rebound patterns and distinguish transient from sustained effects.
Plan for weight regain: Research examining body composition or metabolic outcomes should account for post-treatment weight regain in power calculations and endpoint selection.
Investigate maintenance strategies: Research questions may focus on identifying interventions that prevent or minimize rebound effects, such as continued dietary modification, exercise protocols, or transition to alternative compounds.
Examine individual variability: Some subjects demonstrate less weight regain than others. Identifying predictors of successful weight maintenance after discontinuation represents an important research question.
Comparison with continuous treatment: Study designs comparing continuous versus intermittent semaglutide administration provide insight into whether treatment breaks affect long-term outcomes.
These discontinuation effects underscore that semaglutide produces pharmacological effects requiring continued administration rather than inducing permanent metabolic changes. For researchers examining long-term metabolic interventions, this distinction is critical for interpreting results and designing appropriate protocols.
How is semaglutide different from insulin?
Semaglutide and insulin are fundamentally different compounds with distinct mechanisms. Insulin is a hormone that directly lowers blood glucose by promoting cellular glucose uptake, while semaglutide is a GLP-1 receptor agonist that stimulates glucose-dependent insulin secretion from pancreatic beta cells. Semaglutide does not replace insulin and works only when endogenous insulin secretion capacity exists. In research settings, semaglutide is used to study incretin pathways and metabolic regulation, while insulin is used to study glucose uptake mechanisms and insulin signalling pathways.
Can semaglutide be used in combination with other research compounds?
Yes, semaglutide is frequently used in combination research protocols. Common combinations include pairing with insulin secretagogues, metformin analogues, or other metabolic compounds to examine additive or synergistic effects. Researchers should account for semaglutide’s effects on gastric emptying, which may alter absorption kinetics of co-administered compounds. Combination protocols with other incretin-based compounds (GIP agonists, glucagon agonists) are particularly valuable for dissecting individual receptor pathway contributions to metabolic outcomes.
What is the optimal storage temperature for semaglutide?
Lyophilised (unreconstituted) semaglutide should be stored at -20°C in a freezer, protected from light and moisture, where it remains stable until the expiration date. Once reconstituted with bacteriostatic water, the solution must be stored at 2-8°C (refrigerator) and used within 28 days. Never freeze reconstituted solution, as freezing causes irreversible peptide degradation. Allow refrigerated solution to reach room temperature before injection to minimize injection site discomfort.
How does semaglutide compare to natural GLP-1?
Semaglutide shares 94% sequence homology with native human GLP-1 but incorporates structural modifications that dramatically extend its half-life from approximately 2 minutes (native GLP-1) to 7 days (semaglutide). These modifications include amino acid substitution at position 8 (conferring DPP-4 resistance) and acylation at position 26 (enabling albumin binding). Despite structural differences, semaglutide activates the same GLP-1 receptor and produces similar downstream signalling effects, but with sustained rather than transient activation.
What concentration should I use for semaglutide research?
Concentration depends on research objectives, dosing protocol, and injection volume constraints. Common concentrations range from 1mg/mL to 10mg/mL. Lower concentrations (1-2mg/mL) are appropriate for low-dose protocols or when larger injection volumes are acceptable. Higher concentrations (5-10mg/mL) enable smaller injection volumes for high-dose protocols. Calculate concentration based on: target dose per administration, acceptable injection volume (typically 0.1-0.5mL for subcutaneous injection), and reconstituted solution stability requirements.
Does semaglutide require special handling precautions?
Semaglutide requires standard peptide handling precautions. Use sterile technique during reconstitution and administration to prevent contamination. Protect from light exposure, which may degrade the peptide. Avoid repeated freeze-thaw cycles of lyophilised powder. Never shake reconstituted solution vigorously, as mechanical stress may damage peptide structure. Wear appropriate personal protective equipment (gloves, lab coat) when handling, and dispose of used materials according to institutional biosafety protocols.
Can semaglutide be administered via routes other than subcutaneous injection?
In research settings, subcutaneous administration is standard due to optimal bioavailability and consistent absorption kinetics. Intravenous administration is possible but not typically used due to rapid distribution and lack of advantage over subcutaneous delivery given the long half-life. Oral administration requires specialized formulation with absorption enhancers (as in commercial oral semaglutide products) and is not feasible with standard research-grade compound. Intramuscular injection is not recommended due to unpredictable absorption and potential local tissue reactions.
What is the minimum protocol duration to observe meaningful semaglutide effects?
Minimum duration depends on research endpoints. Acute glucose-lowering effects are observable within 24-48 hours, making single-dose or short-term protocols viable for examining insulin secretion mechanisms. Body weight effects require minimum 8-12 weeks to detect significant changes, with 24-52 week protocols preferred for comprehensive body composition research. Cardiovascular and metabolic marker studies typically require 12-24 weeks minimum. Account for 4-5 weeks to reach steady-state pharmacokinetics when designing protocols examining chronic effects.
How should I calculate dose escalation schedules?
Standard escalation protocols increase dose every 4 weeks, allowing adaptation to gastrointestinal effects before advancing. A typical schedule: 0.25mg weekly × 4 weeks → 0.5mg weekly × 4 weeks → 1.0mg weekly × 4 weeks → 1.7mg weekly × 4 weeks → 2.4mg weekly (target dose). Adjust escalation speed based on research objectives and subject tolerance. Protocols prioritizing rapid target dose achievement may use 2-week intervals, while those prioritizing tolerability may extend to 6-8 week intervals. Include criteria for dose hold or reduction if significant adverse effects occur.
What analytical methods verify semaglutide purity and identity?
High-performance liquid chromatography (HPLC) is the primary method for purity verification, with 99.8% purity standard for research-grade compound. Mass spectrometry confirms molecular weight and identity. Amino acid analysis verifies sequence composition. Peptide content assays quantify actual peptide mass versus total powder mass. Certificates of Analysis from independent third-party laboratories should accompany research-grade semaglutide, documenting these analytical results. Sempica provides CoAs for all compounds, ensuring full transparency and traceability.
Can semaglutide research data be compared across different studies?
Cross-study comparison requires careful attention to protocol differences including dose, escalation schedule, administration timing, subject characteristics, and measurement methods. Semaglutide’s dose-dependent effects mean that studies using different dose ranges may not be directly comparable. Timing of measurements relative to steady-state achievement affects results. Subject baseline characteristics (metabolic status, body composition) influence response magnitude. When comparing studies, document these protocol variables and consider them in interpretation. Standardized protocols and measurement methods improve cross-study comparability.
What documentation is required for semaglutide research protocols?
Comprehensive documentation should include: compound source and lot number, Certificate of Analysis, reconstitution date and method, final concentration, storage conditions, administration dates and doses, injection sites, subject characteristics, baseline measurements, serial outcome measurements, adverse effects, protocol deviations, and post-treatment follow-up data. Maintain detailed laboratory notebooks with dated entries. Document any dose adjustments and rationale. Photographic documentation of injection sites may be valuable for protocols examining local reactions. Proper documentation ensures reproducibility and supports publication.
Semaglutide represents a powerful tool for metabolic research, offering researchers the ability to investigate GLP-1 receptor-mediated pathways and their effects on glucose homeostasis, energy balance, and body composition regulation. As a selective GLP-1 receptor agonist with extended pharmacokinetics, the compound enables once-weekly administration protocols while producing sustained receptor activation and measurable effects across multiple physiological systems.
Understanding what semaglutide is and how it works requires appreciation of its molecular structure, receptor binding characteristics, and downstream signalling cascades. The compound’s effects span immediate glucose-dependent insulin secretion to long-term body weight regulation, with distinct temporal patterns that must inform research protocol design. Proper handling, reconstitution, and administration techniques are essential for reproducible results and subject welfare.
Researchers must recognize semaglutide’s limitations alongside its capabilities. The compound produces pharmacological effects that reverse upon discontinuation rather than permanent metabolic reprogramming. Substantial inter-individual response variability requires flexible protocol designs that accommodate different tolerance and efficacy patterns. Comparison with dual and triple agonist compounds provides context for understanding how additional receptor pathway activation affects metabolic outcomes.
Next steps for researchers:
For laboratories planning semaglutide research protocols, begin with comprehensive protocol design that accounts for dose escalation requirements, appropriate monitoring parameters, and sufficient duration to observe target endpoints. Establish clear research questions that leverage semaglutide’s specific mechanisms rather than generic metabolic effects.
Source research-grade semaglutide from verified suppliers that provide Certificates of Analysis confirming 99.8% purity and proper storage conditions. Sempica supplies high-purity semaglutide with full analytical documentation and global shipping to qualified research professionals.
Implement proper handling protocols including appropriate storage temperatures, sterile reconstitution technique, and correct subcutaneous administration methods. Consult the comprehensive laboratory guide to peptide handling for detailed technical guidance.
Consider comparative research designs that examine semaglutide alongside related compounds such as tirzepatide or retatrutide to dissect individual receptor pathway contributions to metabolic outcomes. These comparative approaches provide mechanistic insight beyond single-compound studies.
Plan for comprehensive data collection including baseline characterization, serial measurements during treatment, and post-treatment follow-up to characterize rebound effects. This complete dataset maximizes scientific value and publication potential.
For research programs examining broader metabolic pathways, explore Sempica’s complete catalogue of metabolic research compounds to identify complementary tools for multi-pathway investigations.
Mandatory Research Use Disclaimer:
Products sold by Sempica are intended for research purposes only. They are not for human consumption, medical use, or therapeutic application. By purchasing from Sempica, you confirm that you are a qualified research professional and will use these products strictly for laboratory research in controlled settings. All research must comply with applicable institutional, local, and national regulations governing laboratory research practices.
Unsure of How much of Ozempic of
Planning to take your first shot of

Are Storing Ozempic in your Refrigerator? How